11 July 2022
In Part 1 of this series, I summarised the four major ways in which COVID-19 injections have interfered with the complex interactions between SARS-CoV-2 and the human immune system, then zoomed in on the first problem: the narrow and short-lived immune response that they generate.
In Part 2 I laid out the evidence that the injections are causing people to become susceptible to repeated infection, most likely through the mechanism of ‘original antigenic sin’, otherwise known as the Hoskins effect and immune imprinting.
And in Part 3, I described the consequences to individuals of the inability to clear viral infection that results from a limited and fixated immune response to SARS-CoV-2.
Finally, in Part 4 I will set what has been discussed in the previous posts into the current global context, explaining why we now have a parade of immune escape variants of SARS-CoV-2 that are turning COVID-19 into the endless pandemic.
Problem #4. COVID-19 injections prevent highly-injected populations from attaining herd immunity and instead select for highly transmissible and (eventually) virulent variants
Let’s start by defining our terms. “Herd immunity” or “community immunity” refers to a state in which a sufficiently large proportion of a population has become immune to a particular infectious disease to prevent widespread transmission of the infectious agent. Herd immunity provides protection against infection to those who have not yet become immune to the disease.
The term “herd immunity” was coined by A. W. Hedrich, after meticulous analysis of the epidemiology of measles in Baltimore from 1900-1931. Hedrich calculated that when more than 55 per cent of children under 15 years of age had become immune to measles via contracting and surviving the infection, measles epidemics ceased. By the end of an epidemic, 30-35 per cent of children under 15 remained susceptible (non-immune).
With only isolated cases of measles occurring, the proportion of non-immune children gradually increased; when it reached 45-50 per cent of children under 15, another measles epidemic was triggered.
Hence, natural measles occurs in waves or cycles of epidemics, with the interval between cycles determined by how long it takes for the pool of ‘susceptibles’ to increase to the level required to trigger an epidemic – 2-3 years in large urban centres.
Despite its origins as a description of a phenomenon induced by the development of natural immunity, the term “herd immunity” has been hijacked by the medical-pharmaceutical-industrial complex which promotes vaccination as the sole means of eradicating infectious diseases (despite abundant evidence that old-fashioned public health interventions such as providing clean water and sewage disposal, adequate nutrition and decent housing largely eradicated the scourge of infectious disease from Westernised countries, long before vaccination campaigns began).
This hijacking reached its zenith (or nadir, depending on how you look at it) in December 2020, when the World Health Organisation (WHO) changed the definition of herd immunity on its website, just before the global roll-out of COVID-19 injections began.
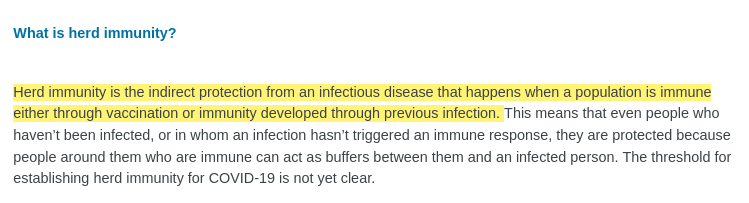
Here’s WHO’s definition of herd immunity from its Coronavirus disease (COVID-19): Serology, antibodies and immunity page, up until 12 November 2020:
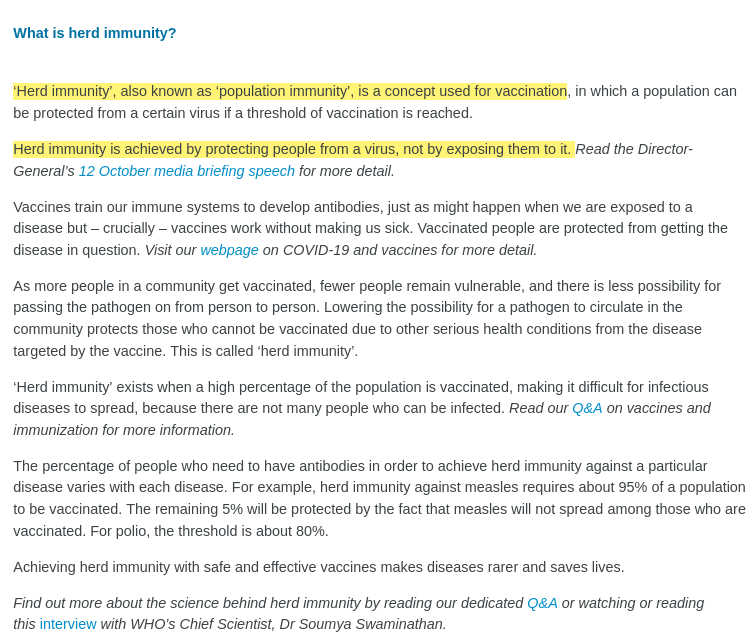
And here’s the version that appeared on 13 November 2020:
In a feat worthy of the Ministry of Truth, WHO attempted to memory hole nearly a century of established biology and epidemiology (not to mention millennia of human experience), expunging the entire concept of natural immunity and entirely appropriating the term “herd immunity” for the vaccine ideology.
(Side note: Did you catch the massive gap between the 55 per cent threshold for herd immunity to measles that Hedrich calculated in the pre-vaccine era, and the 95 per cent target for vaccine-dependent herd immunity? Not to mention the fact that multiple measles outbreaks have occurred in populations with over 95 per cent measles vaccination rates.)
The resulting firestorm of controversy generated by people who had actually read immunology textbooks forced WHO to alter its definition once again, on 31 December 2020:
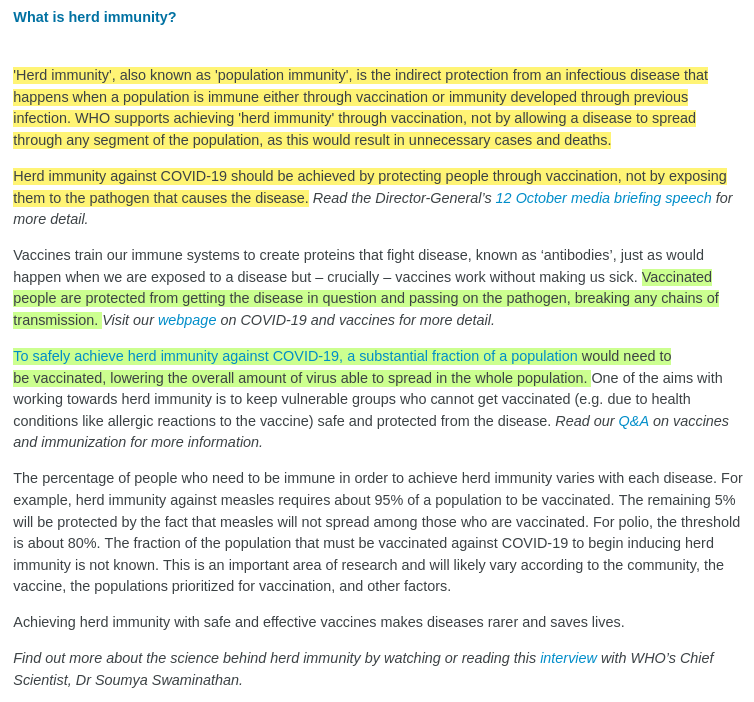
Note how WHO predicates its prejudice against attaining herd immunity through recovery from infection on the premise that “vaccinated people are protected from getting the disease in question and passing on the pathogen, breaking any chains of transmission.”
But as WHO knew perfectly well, none of the clinical trials for COVID-19 injections were set up to ascertain whether the experimental substances prevented infection or transmission, and the definition of “COVID-19” used in these trials was incredibly lax: having even one mild symptom – such as a headache or a cough – along with a positive RT-PCR test result for SARS-CoV-2, qualified participants as having the “disease” of COVID-19. Peter Doshi had penned a stinging editorial on the rank inadequacy of these trials in The BMJ on 21 October 2020, more than two months before the WHO’s weasel-worded second update to its definition of herd immunity.
So how’s that “vaccine”-induced herd immunity to COVID-19 coming along? Well, the triumphant tone of the vaccine promoters has become somewhat more muted of late.
Just last November, Associate Professor James Trauer, who heads the Epidemiological Modelling Unit for the School of Public Health and Preventive Medicine at Monash University, gushed that
“New South Wales is probably the best example of a part of Australia that’s close to herd immunity… They’ve made a huge difference to the epidemic through vaccination, clearly, and that’s been the major thing that’s turned it around in that state. Maybe it’s not quite herd immunity, but it’s pretty close… We’re mostly seeing daily death numbers in the single digits across the country, which is so much better than other countries have managed.”
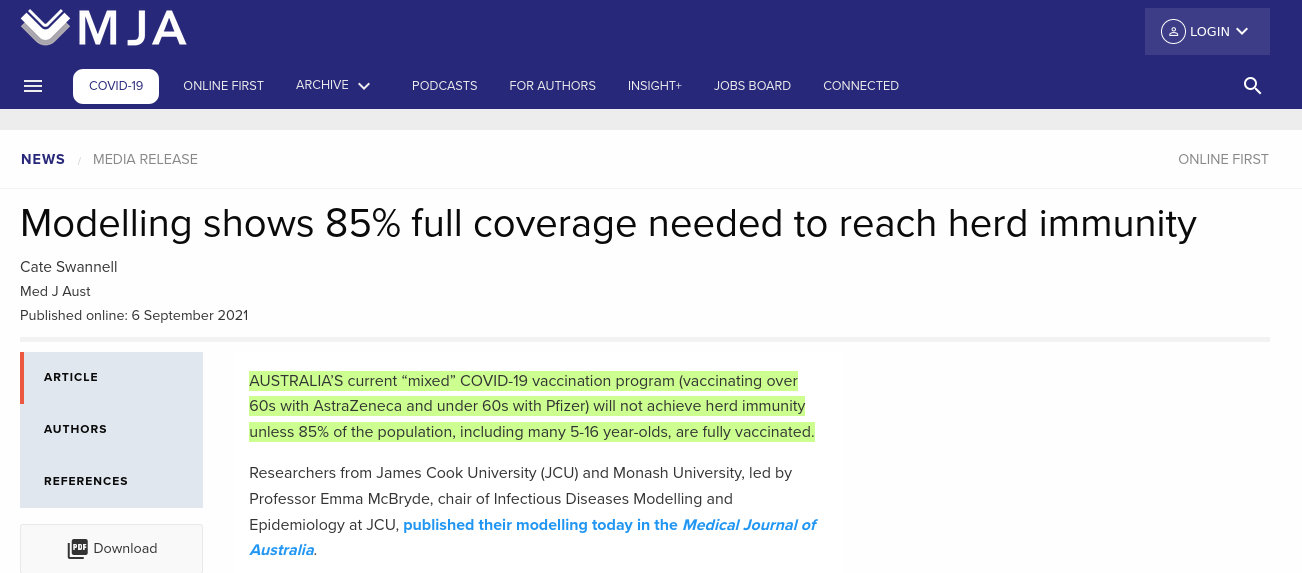
Is the prospect of herd immunity still alive in Australia?
… and then we woke up and smelt the COVID coffee:
What a difference a few months (and a conga line of increasingly transmissible immune escape variants) makes. We’ve gone from this:

and this:

… and this:
… to this:

… and this:
… and this:
… and this:
It’s not just the failure to prevent infection and transmission that has shaken the vaccine true believers out of their herd immunity fever dream. As mentioned in Part 3, by impeding both the innate and acquired arms of the immune system, COVID-19 injections favour the emergence of versions of SARS-CoV-2 that are highly resistant to the incomplete and inflexible immune response that they generate.
And then, as injected people exhale, infectious aerosols containing these immune escape variants are spewed from deep in their lungs, out into the air. In indoor settings with inadequate ventilation and/or low humidity, these aerosols can remain suspended for hours, causing new infections at both short and long ranges.
As also discussed in Part 3, COVID-19 injections impair the clearance of SARS-CoV-2, setting the scene for extended viral replication and the development of many more mutations in the virus’ genetic code, and increasing the probability of variants with tropism for the lung.
According to Muller’s ratchet, ordinarily, mutations that increase transmission are more favourable to the propagation of respiratory viruses than mutations that increase virulence (disease severity). Simply put, a virus that leaves its host well enough to mix with others has a greater chance of spreading itself around than one that renders its host bed-ridden.
However, a virus that doesn’t trigger a robust immune response but does cause extensive shedding of infectious virus can overcome Muller’s ratchet, becoming both highly infectious and – eventually, as it continuously mutates inside its host’s body – highly virulent.
Belgian vaccinologist, Geert Vanden Bossche has described in detail the dire consequences of repeated booster shots on virus-immune system interaction, which may eventually pressure SARS-CoV-2 to completely break through adaptive immune defence. The likely result is antibody-dependent enhancement, the disastrous amplification of infection by injection-induced non-neutralising antibodies, which plagued earlier attempts to develop vaccines against coronaviruses.
According to Vanden Bossche,
“Asymptomatic vaccinees abundantly spread highly infectious SC-2 [SARS-CoV-2] immune escape variants as well as other highly infectious, immunogenically related viruses to other parts of the population. Consequently, in a highly vaccinated, well-mixed population, vaccinees with a mature and healthy innate immune system are now to be considered an asymptomatic reservoir for transmission of new, highly infectious SC-2 immune escape variants and other highly infectious diseases to the remainder of the population.”
Immuno-epidemiologic ramifications of the C-19 mass vaccination experiment: Individual and global health consequences
Remind we, are we seeing immune escape variants? Yes, we are:
“Importantly, BA.2.12.1 and BA.4/BA.5 display stronger neutralization evasion than BA.2 against the plasma from 3-dose vaccination and, most strikingly, from post-vaccination BA.1 infections… post-vaccination BA.1 infection mainly recalls wildtype-induced humoral memory. The resulting elicited antibodies could neutralize both wildtype and BA.1 and are enriched on non-ACE2-competing epitopes. However, most of these cross-reactive NAbs are heavily escaped by L452Q, L452R and F486V.”
BA.2.12.1, BA.4 and BA.5 escape antibodies elicited by Omicron infection
Or, in English, the latest Omicron variants have acquired mutations that help them dodge antibodies induced by the injections. And when people get infected with Omicron after they’ve taken their shots, their immune system churns out antibodies that are matched to the original, now long-extinct Wuhan strain of SARS-CoV-2. These antibodies have some capability of neutralising the original Omicron but not the spin-offs – precisely because the injections are driving the virus to mutate at an ever-faster pace.
“Our data show that BA.2.12.1 and BA.4/BA.5 substantially escape NAbs [neutralising antibodies] induced by both vaccination and infection. Moreover, BA.4/BA.5 NAb titers, and to lesser extent BA.2.12.1 NAb titers, were lower than BA.1 and BA.2 NAb titers, suggesting that the SARS-CoV-2 Omicron variant has continued to evolve with increasing neutralization escape.”
Neutralization Escape by the SARS-CoV-2 Omicron Variants BA.2.12.1 and BA.4/BA.5
Oh yeah, and variant-specific boosters won’t help (and will probably make the situation worse):
“Together, our results indicate that Omicron may evolve mutations to evade the humoral immunity elicited by BA.1 infection, suggesting that BA.1-derived vaccine boosters may not achieve broad-spectrum protection against new Omicron variants.”
BA.2.12.1, BA.4 and BA.5 escape antibodies elicited by Omicron infection
OK, so if Vanden Bossche is correct, we should expect greater spread of the most highly transmissible immune escape variants in populations with higher rates of injection. Like this, perhaps?
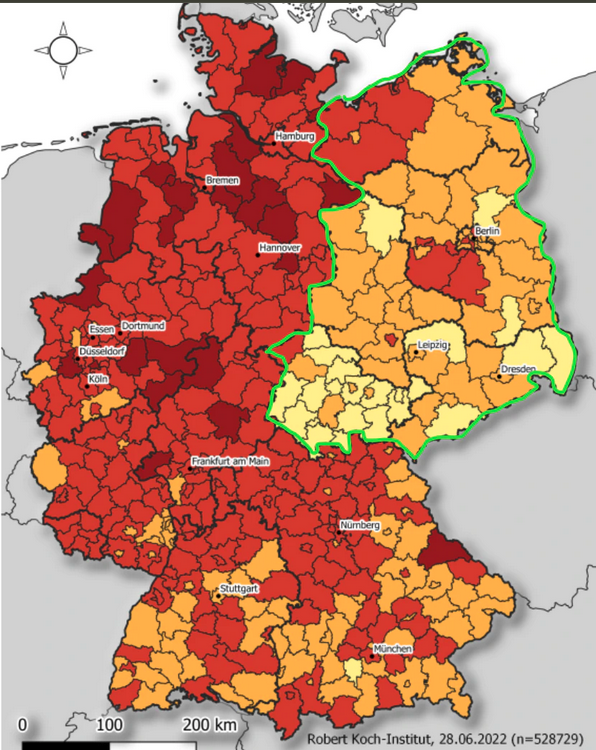
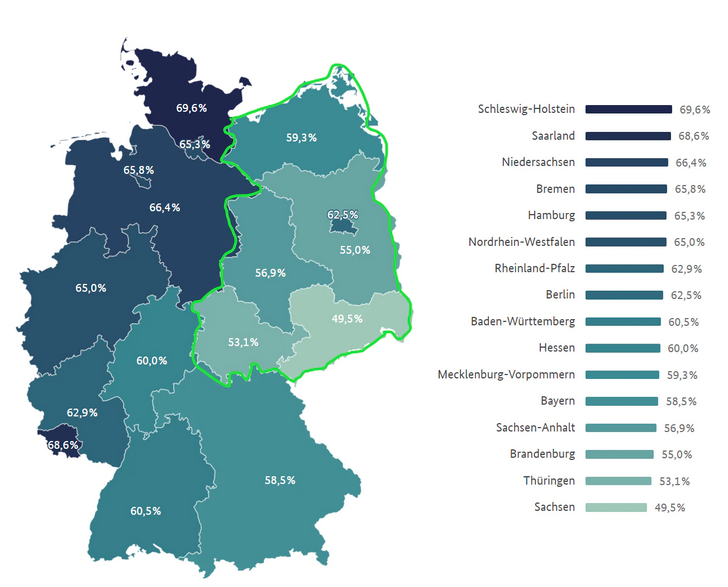
The green lines were drawn in by the German academic who goes by the nom de plume Eugyppius; they mark the boundaries of the old German Democratic Republic – that is, communist East Germany – which was still a thing when I studied German in high school (the Berlin wall fell in my final year). Oddly enough, people who’ve lived under Communism are a tad suspicious of authority, as Eugyppius indicates:
“East Germans have direct experience with government propaganda, and have proven more resistent (sic) to the vaccination campaign than Westerners. Their reward, after being much maligned by state media, is now higher levels of natural immunity and lower rates of BA.5 infection, which appears to prefer vaccinated populations.”
Omicron BA.5 Prefers Hypervaccinated Masking West Germans, Avoids the Former DDR
You can also read Eugyppius’ explication of the progression of both the pandemic and the injection campaigns in the former West and East Germany here, and his pungent response to the lamestream media sock puppets’ (yep, they have them in Germany too) attempt to “debunk” him here.
Back to Vanden Bossche:
“The resulting enhanced viral transmission rate is likely to ignite new pandemics, not only of new, highly infectious, and antigenically shifted SC-2 variants (typically labeled as ‘variants of concern’) but also of avian influenza virus and monkeypox virus.”
Immuno-epidemiologic ramifications of the C-19 mass vaccination experiment: Individual and global health consequences
Hmmm, so maybe, perhaps, just possibly we might see something kinda, sorta, just vaguely like Australia’s current horror flu season?
According to The Guardian,
“Australia has had its worst May on record when it comes to flu cases… The national disease surveillance system reported about 65,770 confirmed influenza cases in May – more than double the month’s previous record, which was set in 2019.
As of 5 June, the national surveillance system had this year received nearly 88,000 reports of flu cases – more than 47,800 of them, diagnosed in the previous fortnight.
The system was notified of 27 flu-related deaths in the year to date, and more than 730 people were reported as admitted to hospital because of influenza since April. Of those hospital admissions, about 6% went directly to intensive care.”
Australia’s monthly flu cases more than doubled previous record in May
(Side note: Of course, the Bill Gates-funded Guardian pushes influenza vaccination as the solution to this unfolding disaster, despite the Cochrane review concluding that it reduces the absolute risk of influenza in healthy adults by 1 per cent and likely has “little or no appreciable effect on hospitalisations”.
In addition, a study examining the shedding of infectious influenza virus in the exhaled breath of flu patients found that “fine-aerosol viral RNA was also positively associated with having influenza vaccination for both the current and prior season.” That is, people who had taken both last season’s and the current season’s flu jab shed more highly infectious virus particles in their breath than those who had not been vaccinated. The real superspreaders are those who obediently line up for their flu shot every year.)
Vanden Bossche goes on to propose that
“As currently circulating Omicron (sub)variants become more and more resistant to potentially virulence-neutralizing vaccinal Abs… infection by these variants will rapidly become highly virulent in vaccinees, but not in the unvaccinated.”
Immuno-epidemiologic ramifications of the C-19 mass vaccination experiment: Individual and global health consequences
If Vanden Bossche’s hypothesis is correct, here’s what we can expect to see:
“As the second viral immune escape event (enabling ADED [antibody-dependent enhanced disease]) does not affect the unvaccinated, the proportion between vaccinated and unvaccinated people needing hospitalization because of severe C-19 disease is expected to rise rapidly in the age group between 10 and 60 years… This will be the most sensitive, and hence, first measurable signal of the evolution of SC-2 toward an infectious behavior that will be responsible for initiating a massive ADED-mediated incidence of severe disease and hospitalization in the overall vaccinated part of the population.”
Immuno-epidemiologic ramifications of the C-19 mass vaccination experiment: Individual and global health consequences
And then:
“The case fatality rate in the vaccinated population will rapidly and dramatically increase, first in the vaccinated elderly (+ the vulnerable) and soon thereafter also in the rest of the vaccinated population.”
Immuno-epidemiologic ramifications of the C-19 mass vaccination experiment: Individual and global health consequences
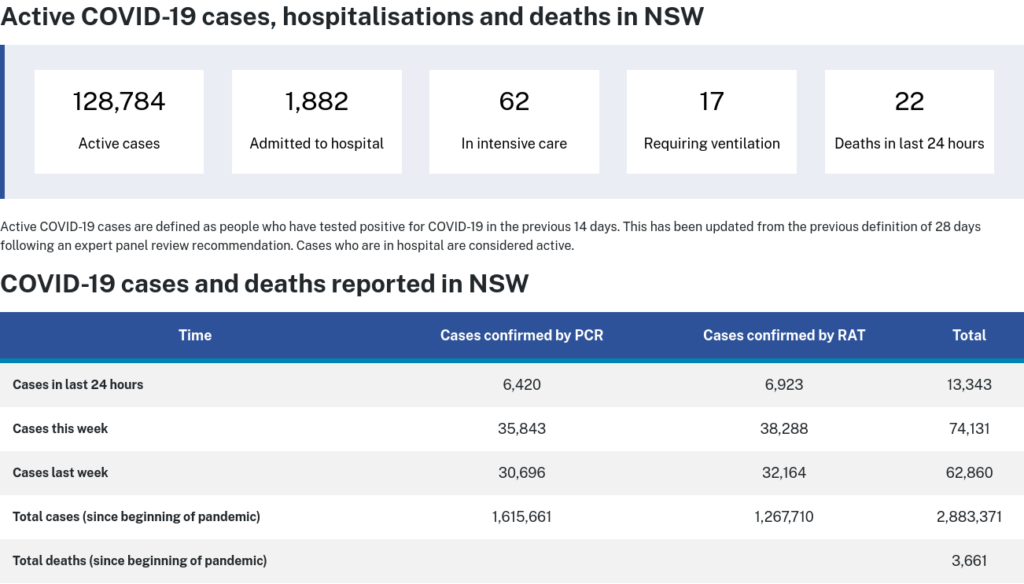
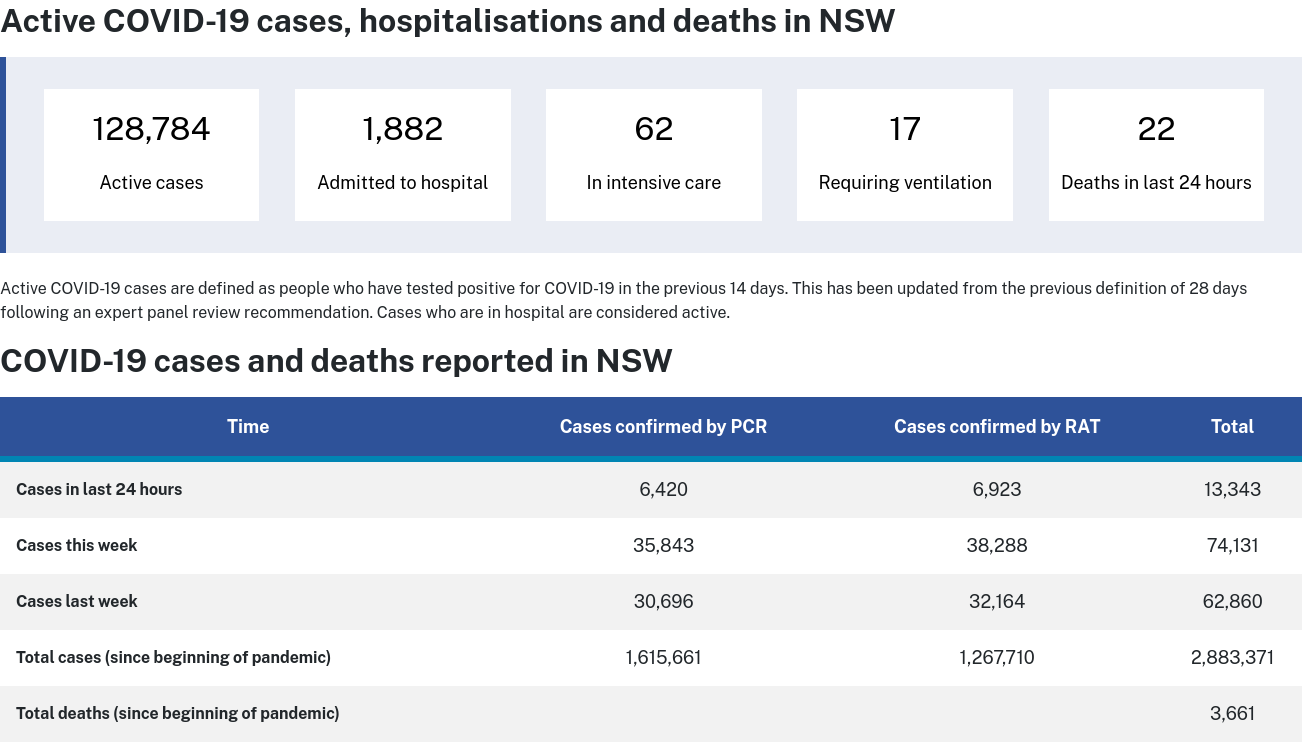
Hmmm, rising hospitalisation and death rates in highly injected populations – you mean as highly injected as this?
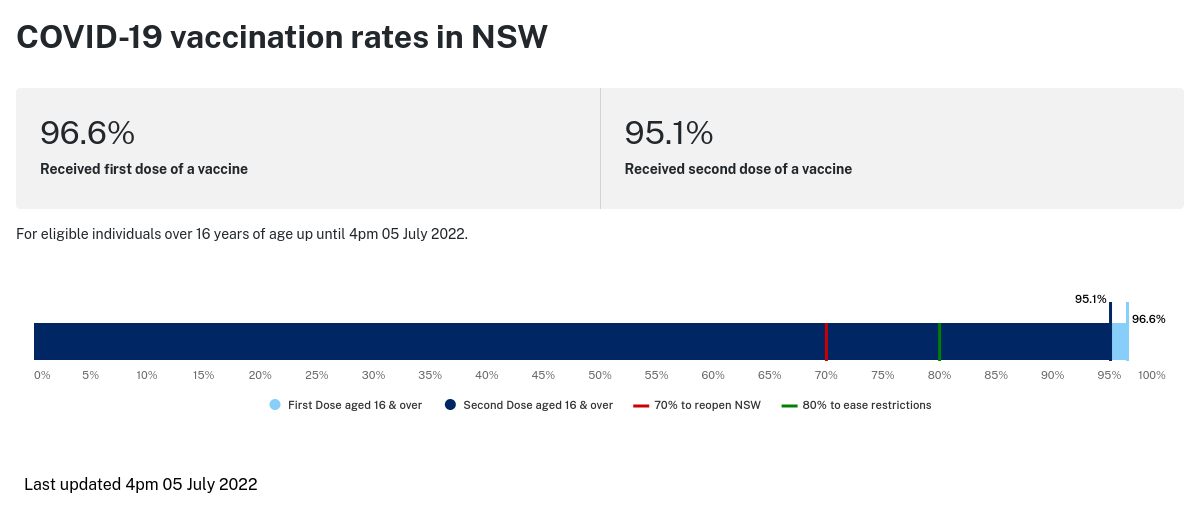
Let’s look at how NSW is doing again:
Let’s set that in the context of the injection roll-out, shall we?
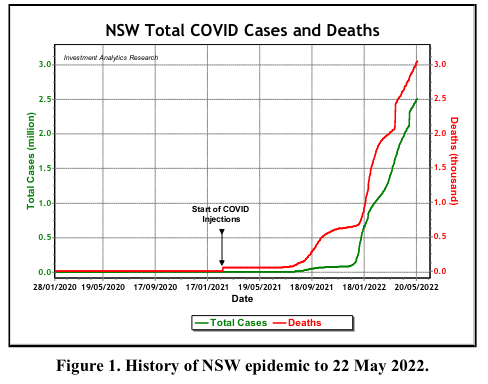
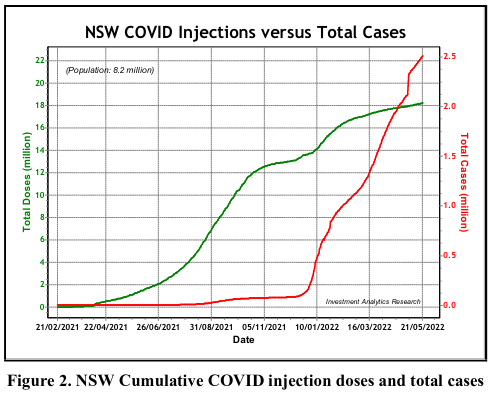
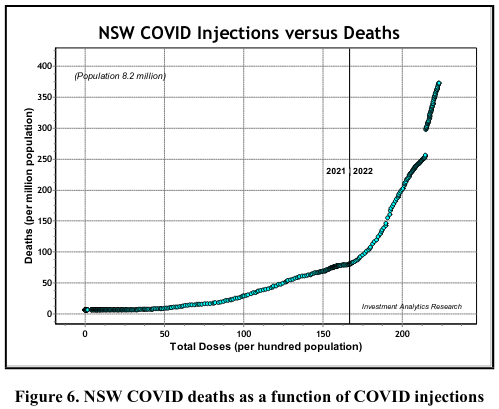
Let’s recap. To fulfil Geert Vanden Bossche’s prophecy of COVIDoom, we would have to be observing immune escape variants of SARS-CoV-2 proliferating and concentrating in highly-injected populations, developing mutations that facilitate greater and greater capacity to evade injection-induced antibodies, until they eventually break Muller’s ratchet and become both infectious and virulent. At this point we would see not only rising hospitalisation and death rates from COVID-19, but from other infectious diseases such as influenza.

What can be done to avert this impending catastrophe?
- Stop jabbing now. If you’ve already had one, or two, or three or (god forbid) four, stop. If you haven’t had any yet, don’t even think about it (and if you’re tempted by Novavax because “it’s not like the others”, read this first). As for jabbing your kids, I don’t mean to be rude, but you’d have to be out of your freakin’ mind.
- If you have already had a COVID-19 injection, familiarise yourself with evidence-based prevention and early treatment protocols (these are the ones I recommend) and make sure you have everything you need on hand. Ditto if you’re unjabbed but have loved ones who are – they may think you’re a tinfoil hat-wearing antivaxxer conspiracy theorist now, but they might just thank you later.

- Support your immune system’s ability to defend you against infectious disease by taking responsibility for your own health. It’s not your doctor’s job to keep you healthy, it’s yours. Delegating the responsibilities of adulthood to ‘authorities’ is how we got ourselves into this mess in the first place. If we’re ever going to extricate ourselves from it, we all have to grow up and stop making excuses for why we eat crap, sit on our butts all day staring at our devices, and let our kids be propagandised by ideologically possessed muppets (no offence meant to the original Muppets, whom I dearly love). I have a library of fully-referenced articles on cultivating healthy immune function here; you might like to start with Nutrition and your immune system. Oh, and get outside too.
Summing up
The COVID-19 injection program has been an unmitigated disaster. It has interfered with the development of robust, broad and durable immunity to SARS-CoV-2 in individuals and sabotaged the development of herd immunity. It has thrown a giant monkey wrench into the complex interrelationship between virus and host, sparking an evolutionary arms race in which what should have been a low-consequence flu-like respiratory virus is now poised to break Muller’s ratchet and become both highly transmissible and highly virulent.
There are many things we need to learn from this dark episode in human history, but the most important of them can be summed up in this classic number from one of my favourite bands:




