25 July 2022
As I’ve mentioned in previous articles, psychiatry has a validity problem. In science, validity refers to the extent to which a concept, conclusion or measurement is well-founded and likely corresponds accurately to the real world. If an experiment is valid, its results really do measure the concept being tested. If a diagnosis is valid, it is grounded in biological reality1.
As even the former director of the US National Institutes for Mental Health (NIMH), Thomas Insel, admitted back in 2013, psychiatric diagnoses suffer from a “lack of validity”.
Insel set the science cat among the pharmaceutical-medical-industrial complex pigeons by announcing that NIMH – the largest funder of research on “mental illness” in the world – would be “re-orienting its research away from DSM categories” because of this lack of validity.
The DSM, or Diagnostic and Statistical Manual, is often described as the Bible of the field of psychiatry. As Insel pointed out, however, “it is, at best, a dictionary, creating a set of labels and defining each.”
The problem Insel identified is that the definitions of all these supposed mental and psychological disorders are based on symptoms, descriptions and markers of conditions – in other words, they’re vague and highly subjective:
“Unlike our definitions of ischemic heart disease, lymphoma, or AIDS, the DSM diagnoses are based on a consensus about clusters of clinical symptoms, not any objective laboratory measure. In the rest of medicine, this would be equivalent to creating diagnostic systems based on the nature of chest pain or the quality of fever. Indeed, symptom-based diagnosis, once common in other areas of medicine, has been largely replaced in the past half century as we have understood that symptoms alone rarely indicate the best choice of treatment. Patients with mental disorders deserve better.”
Psychiatry in Crisis! Mental Health Director Rejects Psychiatric “Bible” and Replaces With Nothing
Insel announced that NIMH would be replacing the DSM with “Research Domain Criteria (RDoC)“, which define mental disorders not through lists of signs and symptoms but instead using more specific genetic, neural and cognitive data.
However, he then went on to admit that “we cannot design a system based on biomarkers or cognitive performance because we lack the data” [emphasis added].
The significance of Insel’s statements on the lack of objective evidence for so-called mental illnesses and disorders cannot be overstated. It reveals the entire field of psychiatry, and the psychopharmacology that has been its therapeutic mainstay since the 1950s, to be a giant fraud. Insel was essentially admitting not only that psychiatric diagnoses lacked validity, but that, therefore, there was no biologically valid theoretical basis for the use of psychiatric drugs.
So, did the replacement of DSM labels with RDoC generate an explosion of knowledge on the biological basis of “mental illness”, resulting in greatly enhanced diagnostic accuracy and an explosion of evidence-based, rational treatments? Hell, no. Psychiatry today is the same shell game as it ever was.
Let’s take attention-deficit/hyperactivity disorder (ADHD) as an example.
According to psychiatrists, ADHD is “a neuro-developmental disorder, characterised by developmentally inappropriate levels of inattention, hyperactivity and impulsiveness”. Remarkably, given that children follow the same neurodevelopmental trajectory no matter where they are born, the global prevalence of ADHD varies widely, from 2 per cent to 7 per cent. In the US, roughly 9 per cent of children have been “diagnosed” with ADHD at some point in their lives.
Here are the diagnostic criteria for this supposed condition, according to the DSM-V:
- Inattention: Six or more symptoms of inattention for children up to age 16 years, or five or more for adolescents age 17 years and older and adults; symptoms of inattention have been present for at least 6 months, and they are inappropriate for developmental level:
- Often fails to give close attention to details or makes careless mistakes in schoolwork, at work, or with other activities.
- Often has trouble holding attention on tasks or play activities.
- Often does not seem to listen when spoken to directly.
- Often does not follow through on instructions and fails to finish schoolwork, chores, or duties in the workplace (e.g., loses focus, side-tracked).
- Often has trouble organizing tasks and activities.
- Often avoids, dislikes, or is reluctant to do tasks that require mental effort over a long period of time (such as schoolwork or homework).
- Often loses things necessary for tasks and activities (e.g. school materials, pencils, books, tools, wallets, keys, paperwork, eyeglasses, mobile telephones).
- Is often easily distracted
- Is often forgetful in daily activities.
- Hyperactivity and Impulsivity: Six or more symptoms of hyperactivity-impulsivity for children up to age 16 years, or five or more for adolescents age 17 years and older and adults; symptoms of hyperactivity-impulsivity have been present for at least 6 months to an extent that is disruptive and inappropriate for the person’s developmental level:
- Often fidgets with or taps hands or feet, or squirms in seat.
- Often leaves seat in situations when remaining seated is expected.
- Often runs about or climbs in situations where it is not appropriate (adolescents or adults may be limited to feeling restless).
- Often unable to play or take part in leisure activities quietly.
- Is often “on the go” acting as if “driven by a motor”.
- Often talks excessively.
- Often blurts out an answer before a question has been completed.
- Often has trouble waiting their turn.
- Often interrupts or intrudes on others (e.g., butts into conversations or games)
Do these sound like symptoms of a “neurodevelopmental disorder” to you, or a litany of parents’ and teachers’ complaints about quintessentially childish characteristics that they find inconvenient, irritating and disruptive?
Well, here’s a clue:
The youngest children in the class are the most likely to be diagnosed with ADHD
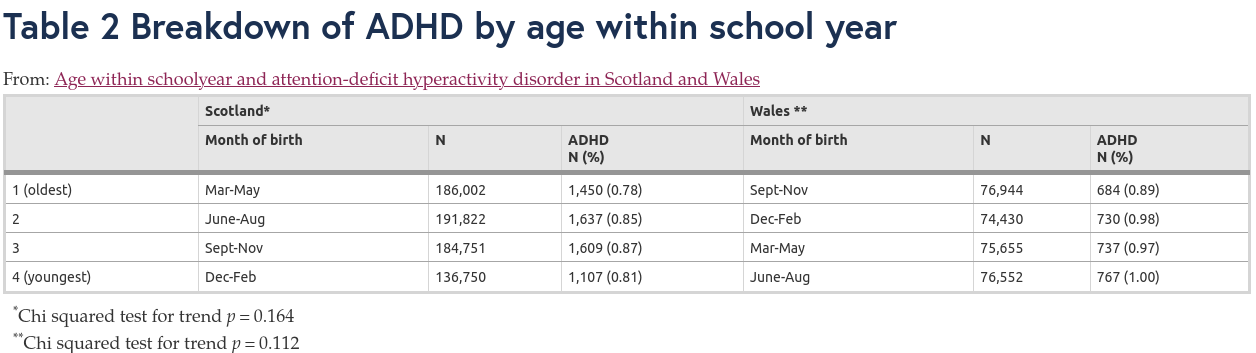
Building on previous studies that found that children who were the youngest in their school year had higher rates of diagnosis with ADHD, researchers analysed data from over a million school children in Scotland and Wales.
These two countries within the UK have different birthday cut-offs for school entry (1st March for Scotland vs 1st September for Wales) and different policies for holding back children whose birthdays fall within the eligibility range for school entry, but are considered too developmentally immature to start school. Scottish children are ten times more likely than Welsh children to be held back for a year if they would otherwise be among the youngest in the year.
Hence, whilst the prevalence of diagnosed ADHD in Welsh schoolchildren was lowest in the children who were the oldest in their school year, and highest in the youngest children, in Scotland, “the prevalence of ADHD increased from the oldest quartile to the second youngest, but then fell in the youngest quartile”:
However, after the researchers adjusted their data for the Scottish holding-back policies, they found that
“If the children who were held back a year had been in their expected schoolyear, the prevalence of ADHD in Scotland across the four quartiles from oldest to youngest would have been: 0.79%, 0.89%, 0.97% and 1.01% (chi trend, p < 0.001).”
Age within schoolyear and attention-deficit hyperactivity disorder in Scotland and Wales
In other words, the relationship between relative age within school year and ADHD was restored once Scotland’s holding back policies were accounted for.
The researchers concluded that
“Children younger within schoolyear are more likely to be treated for ADHD, suggesting immaturity may influence diagnosis.”
Age within schoolyear and attention-deficit hyperactivity disorder in Scotland and Wales
In other words, teachers and parents are more likely to view the behaviour of children with younger relative age within a class as being “developmentally inappropriate” and therefore indicative of ADHD. But the youngest children in a class may be a full year younger than the oldest, and a year is a long time in child development!
On the basis of these ill-informed parental and teacher judgements, millions of children who are simply immature have been stigmatised as suffering from a “developmental disorder”, and prescribed potent psychostimulant medications.
But if ADHD is a genuine neurodevelopmental disorder, shouldn’t there be a more reliable way of distinguishing it from simple developmental immaturity?
Is ADHD a biological disorder?
If ADHD was truly a biological disorder, you would expect there to be identifiable, measurable differences in the brains of children who had it.
Yet when researchers at Duke University performed MRI scans on the brains of over 10 000 children aged 9-10, 949 of whom met the diagnostic criteria for ADHD, they found only minor differences in the brains of the kids who supposedly had this disorder:
“In the full model, which included potential confounding variables selected a priori, we found only 11 significant differences across the 79 brain measures after false discovery rate correction, all indicating reductions in brain measures among participants with ADHD. Cohen’s d values were small, ranging from −0·11 to −0·06, and were not meaningfully changed by using a more restrictive comparison group or alternative diagnostic methods. Simulations indicated adequate statistical power to detect differences even if there was substantial diagnostic misclassification.”
Structural brain measures among children with and without ADHD in the Adolescent Brain and Cognitive Development Study cohort: a cross-sectional US population-based study
For those not familiar with statistics, a Cohen’s d value of 0.8 is considered a large effect size, 0.6 is a medium effect size and 0.2 is a small effect size. So the effect sizes found in this study were really bloody tiny and therefore, unlikely to be useful in diagnosing the so-called condition (as the researchers themselves acknowledged).
The failure of the study to identify any brain-based biomarker of ADHD did not change the conviction of the study’s lead author, Jonathan Posner, MD that ADHD is indeed a biological condition. Posner, perhaps not coincidentally, is a member of The Sackler Institute for Developmental Psychobiology founded by Mortimer Sackler, of the infamous Sackler family largely responsible for the opioid epidemic that has cost the lives of nearly half a million Americans.
According to their website, “The Institute is the product of the vision of Mortimer D. Sackler, MD who saw the need to better understand the developmental processes leading to health and disease.” That sounds like a worthy mission, until you reflect on the fact that the Sackler’s family company, Purdue Pharmaceuticals, framed its mission as helping physicians and the public “understand” the (non-existent) problem of undiagnosed and undertreated pain. This is how the Sackler family justified Purdue’s aggressive marketing of highly addictive opioid drugs like OxyContin. So forgive me for being just a little cynical of Mortimer Sackler’s motives; I’m not sure that the word “understand” means the same thing to you and me as to members of the Sackler family.
Referring to the debate over whether ADHD is truly a biological disorder or simply a reflection of normal variation in attention, Posner averred:
“While this finding rekindles that long-standing debate, we do believe it is a biological disorder… It can be both—a biological disorder, but also have normal variations within that.”
MRI Scans Show Few Brain Differences in Children With ADHD
Got that? Sure, there is normal variation in attention-related behaviour between kids, but even though there are no major differences in the brains of kids who are down the low end of the attention bell curve, we believe that they really do have a “biological disorder” anyway. Because Science™.
Posner and his coauthors urged other true believers in the biological basis of ADHD to keep scouring the land for the footprints of the mythical beast they had failed to find:
“Future studies might need to incorporate other MRI modalities, novel statistical approaches, or alternative diagnostic classifications, particularly for research aimed at developing ADHD diagnostic biomarkers.”
Structural brain measures among children with and without ADHD in the Adolescent Brain and Cognitive Development Study cohort: a cross-sectional US population-based study
Or, in other words, “we just torched tens of thousands of taxpayers’ dollars in grant money and found diddly squat, but we’re going to keep riding this gravy train anyway rather than question our underlying premise that these kids have something wrong with their brains.”
In a press release for the study, Posner stressed that “it’s important to note that ADHD can be impairing” and that “treatments help with that”.
By treatments, of course, Posner means drugs. Specifically, central nervous stimulants such as methylphenidate (Ritalin, Concerta), dextroamphetamine/amphetamine (Adderall) and dexmethylphenidate (Focalin), which are the most frequently-prescribed medications for this “condition”.
These drugs all have significant potential to cause abuse and dependence, and trying to get off them can trigger withdrawal symptoms such as severe tiredness, sleep problems, and mental/mood changes such as depression.
The prescribing information for these drugs is highly revealing; the manufacturers essentially admit that the diagnostic criteria for ADHD are flimsy, no one really knows how the drugs ‘work’, they haven’t been tested for efficacy past a couple of months despite almost always being prescribed long-term, and it’s up to doctors to determine whether the patient can go off them, by assessing their “functioning”… whatever that means, in the absence of a valid diagnostic test!
For example, here are some excerpts from the prescribing information for Concerta:
“Specific etiology of this syndrome [ADHD] is unknown, and there is no single diagnostic test…
There is no body of evidence available from controlled trials to indicate how long the patient with ADHD should be treated with Concerta®. It is generally agreed, however, that pharmacological treatment of ADHD may be needed for extended periods.
The effectiveness of Concerta® for long-term use, i.e., for more than 7 weeks, has not been systematically evaluated in controlled trials. The physician who elects to use Concerta® for extended periods in patients with ADHD should periodically re-evaluate the long-term usefulness of the drug for the individual patient with trials off medication to assess the patient’s functioning without pharmacotherapy. Improvement may be sustained when the drug is either temporarily or permanently discontinued.”
Concerta – drugs.com
The justification for prescribing dangerous mind-altering and heart-damaging drugs (for which there’s now a thriving black market) to schoolchildren as young as six is that by settling down their restless minds and bodies, stimulants help kids learn better. But is this true?
Psychostimulants don’t enhance learning or academic outcomes
It’s remarkable that the claim that stimulant drugs improve children’s ability to learn has never actually been put to the test, until researchers from the Center for Children and Families at Florida International University conducted this study.
In an elegant study design, 173 children aged 7-12, who met DSM-5 criteria for ADHD, took part in a triple-masked, within-subject, AB/BA crossover trial. Children undertook two consecutive 3-week phases of daily, 25-minute small-group instruction in both (a) subject-area content (science, social studies) and (b) vocabulary. They took methylphenidate during one of these phases, and a placebo during the other, so each child served as their own control. Neither the children, their parents nor the instructors knew whether the children were taking the drug or placebo.
The stimulant drug was highly effective at increasing the time that children spent sitting in their seats and staying focused on their tasks, and at improving their classroom behaviour:
“When taking medication, children completed 37% more arithmetic problems per minute and exhibited 53% fewer classroom rule violations per hour.”
ADHD: Medication alone doesn’t improve classroom learning for children – new research
But the kids didn’t learn any more of the science, social studies, and vocabulary content during the periods they were taking these drugs:
“In this controlled study, there was no detectable impact of extended-release methylphenidate on the learning of units of academic material taught via small-group, evidence-based instruction. Methylphenidate improved seatwork productivity and classroom behavior, as in many previous studies, but these benefits did not translate into improved learning of academic material.”
The effect of stimulant medication on the learning of academic curricula in children with ADHD: A randomized crossover study
Can you even wrap your mind around this travesty? Children are being prescribed powerful and dangerous stimulant drugs in order to make teachers’ (and parents’) jobs easier by zonking them out so they sit still, stop disrupting other kids, and give the illusion of paying attention to their work, while receiving no benefit to their academic performance and hence their life prospects.
It’s bad enough that stimulant drugs are all risk and no benefit for kids; the fact that they’re prescribed for a “condition” for which no biological basis has been found, just adds insult to injury.
Speaking of injury, can you guess which drug, recommended by doctors for fevers and pain relief during pregnancy, increases the risk of genuine neurodevelopmental disorders?
Paracetamol – bad for bubs’ brains (and bodies)
A review of 25 years of research in humans, animals and in vitro on the prenatal use of paracetamol (known in the US as acetaminophen), concluded that the children of mothers who took this over-the-counter drug whilst pregnant with them were more likely to be diagnosed with ADHD and autism, and to have a lower IQ. Girls whose mothers took paracetamol during their pregnancy were also found to have a higher risk of language delays and early onset of puberty, whilst boys showed indicators of disturbed masculinisation including a higher risk of undescended testicles (cryptorchidism) and reduced anogenital distance.
And, in stark contrast to the lack of evidence for a biological basis for generic “ADHD”, research has revealed a neurobiological link between exposure to paracetamol during gestation (obviously a critical time for the formation of all organs including the brain), and functional alterations in children’s brains.
Specifically, children who were found to have paracetamol in their meconium (first bowel movement), indicating that their mothers had taken the drug whilst pregnant with them, were not only nearly 2.5 times more likely to be diagnosed with ADHD by the age of 9-11 years, but there was a dose-response relationship: each doubling of exposure increased the odds of an ADHD diagnosis by 10 per cent.
Using functional MRI scanning, researchers found a neurobiological correlate of in utero exposure to paracetamol which helped to explain the children’s behaviour:
“Children with acetaminophen detected in meconium showed increased negative connectivity between frontoparietal and default mode network nodes to clusters in the sensorimotor cortices, which mediated an indirect effect on increased child hyperactivity.”
Association of Prenatal Acetaminophen Exposure Measured in Meconium With Risk of Attention-Deficit/Hyperactivity Disorder Mediated by Frontoparietal Network Brain Connectivity
The frontoparietal network is involved in executive function, otherwise known as cognitive control – the higher-level cognitive skills that help us organise our thoughts and activities, prioritise tasks, manage time efficiently, and make decisions.
The default mode network is a system of connected brain areas that show increased activity when a person is not focused on what is happening around them, such as when daydreaming.
By screwing up the connections between these vital brain regions and the regions which process sensory inputs and decide on responses to them, prenatal exposure to paracetamol appears to make children more hyperactive.
So we have a drug that is recommended by drug regulators and doctors for use in pregnancy, and is taken by roughly 50 per cent of pregnant women worldwide (and up to 65 per cent of pregnant women in the US), which appears to be causing brain injuries in children that result in disruptive behaviour for which powerful brain-altering stimulants are prescribed, usually for many years and even decades. A cynical person might conclude that this is all a giant racket.
Finding hope in the produce aisle
What’s a parent to do if their child’s inability to focus their attention is causing problems at home and in school? According to the Micronutrients for ADHD in Youth (MADDY) Study, the higher the intake of fruits and vegetables, the lower the severity of inattention in children diagnosed with ADHD.
Given the vast pre-existing literature on the benefits of fruit and vegetable consumption for various aspects of cognitive function, this finding points, once again, to possible biological mechanisms for certain challenging behaviours in children that are attributed to “ADHD”.
Does it make more sense to label kids who have trouble paying attention because their brains are deprived of nutrients found in fresh produce as suffering from a “neurodevelopmental disorder”, or a dietary deficiency?
Of course, not all inattentiveness in children is attributable to dietary factors – but that’s just the point.
There are a multitude of reasons why children might be inattentive, hyperactive, disruptive, disorganised, or frequently bored. Poverty, poor nutrition, family violence, lack of parenting skills, a mismatch between the child’s learning style and educational environment, insufficient sleep, excessive use of devices, nature deficiency, brain damage from in utero exposure to alcohol or drugs, and plain old immaturity are just some of these reasons.
Throwing children into the “wastebasket diagnosis” of ADHD does absolutely zero to address any of these underlying drivers of behaviour. Even worse, being diagnosed with ADHD is frequently a one-way ticket on the stimulant drug train, which for many kids, ends up being a journey straight to hell:
Back in 2013, Thomas Insel wrote that “patients with mental disorders deserve better” than the DSM-guided practice of psychiatry was offering them.
I would go one step further. We need to stop thinking of “conditions” such as ADHD as being “mental disorders”, and instead approach all children and all adults who are struggling to live productive, fulfilling lives as individuals who require holistic assessment and a whole-of-life approach to solving their problems.
In my clinical practice, I have found that I can get the best results for my clients using a synthesis of the insights gained by evolutionary psychology and personality psychology to provide a framework for understanding the problems of living, and Lifestyle Medicine along with techniques for change developed by energy psychology to address them. This client-centred approach is the polar opposite of psychiatry’s cookie cutter process of diagnosis and treatment.
Which approach should you take, if you or a loved one has been diagnosed with ADHD or some other “mental disorder” or “neurodevelopmental disorder”? It’s up to you, of course, as all your healthcare choices should be.
But before you choose which course of treatment to follow, you should know that since psychiatry embraced psychopharmacology in the late 1950s, there has been a dramatic explosion in the number of adults and children disabled by “mental illness”, as Robert Whitaker painstakingly documented in his paradigm-smashing book Anatomy of an Epidemic. Does that prove that psychiatry is a fraud, and diagnoses such as ADHD are a scam? You be the judge.
Update: One of my readers, Peter Tomkinson shared (https://robynchuter.substack.com/p/the-adhd-scam-podcast/comment/7937258) a link to a powerful presentation by Dr James Davies, which summarises his eye-opening book Cracked: Why Psychiatry is Doing More Harm Than Good. I read the book several years ago, and it vastly enhanced my understanding of what is wrong with psychiatry.
You can watch the presentation here:
To learn more about how Lifestyle Medicine interventions such as improved nutrition, physical activity, nature therapy, and effective psychotherapy can help people diagnosed with ADHD, apply for a Roadmap to Optimal Health Consultation today.
- This is one of the key elements of the COVID-19 fraud. A person who tests positive to the presence of SARS-CoV-2, but has no signs or symptoms of respiratory tract infection, does not “have COVID” because COVID-19 – short for COronaVIrus Disease 2019 – is by definition a disease, and a person who has no symptoms of respiratory tract infection by definition does not have that disease. ↩︎



