As I discussed in a previous article, we are constantly being told by politicians, the media, and now ‘celebrities‘, that we are ‘at war’ with the novel coronavirus dubbed SARS-CoV-2.
The virus did not declare war on us. Viruses are not living organisms and therefore are not capable of forming intentions or acting upon them; they simply move from host to host in order to perpetuate themselves, adapting as they go.
No, we declared war on the virus. And any party which declares war should have a clear objective for that war. How else would one know that the war had been won, so that all the resources (financial, intellectual, technological and human) that have been diverted into the war effort can be stood down, and normal civilian life can be resumed?
But what exactly is the objective of the war on SARS-CoV-2?
Initially, we were told that we must all obey social distancing regulations in order to ‘flatten the curve’, so as to avoid overwhelming the health care system.
It’s important to understand that ‘flattening the curve’ doesn’t mean reducing the total number of cases (i.e. people diagnosed with the disease). It means delaying the spread of the virus so that infections are spread out over a longer period of time. The area under the pink and blue curves below represents the number of cases if either nothing is done to delay the spread (pink) or mitigation measures such as social distancing are employed (blue). The number of people infected ends up being essentially the same, no matter which strategy is pursued:
In theory, flattening the curve may reduce the number of deaths from the infection because if too many sick people require health care at once, they may receive inadequate treatment and some of them may die as a consequence.
In reality, flattening the curve may increase the death rate if those at highest risk need to be isolated for a protracted period, due to the impact of the isolation itself. A sad case in point is the death of 109 year old Francesca Placereani, formerly the oldest woman in the Swiss canton of St Gallen. She did not contract the virus and was reported to have been doing well for her age. However,
“She faded without the daily visits of her family members.”
In any case, if flattening the curve was the objective of Australia’s ‘war on the virus’, then we can safely declare Mission Accomplished. According to the Commonwealth Department of Health, as of the time of writing this article (21 May 2020), there are 43 people in hospital for treatment of COVID-19 across the entire nation, and 9 of them are in ICU. I think it’s safe to assume that our healthcare system can cope with this patient volume.

In fact the total number of people hospitalised with COVID-19 since the epidemic began is 866, so at no point was our health care system ever in danger of overwhelm.
But now the objective of the war appears to have changed. According to the signs placed in the playgrounds near my home, and on the walls of the supermarket, we still need to maintain social distancing in order to ‘slow the spread’ of the virus.
How would we know if this objective had been achieved? By examining the number of new cases diagnosed, and the rate of incline or decline in those case notifications. OK, here are the official numbers:

As you can see, the number of new cases of the virus has been slowing down since 28 March, and possibly since 24 March 2020 (the spike in the number of reported cases on 28 March may have been due to a surge in testing or delayed reporting of test results), since all epidemics follow Farr’s Law:
“Epidemics rise and fall in roughly a bell-shaped curve (a normal distribution) shape. Farr shows us that once peak infection has been reached then it will roughly follow the same symmetrical pattern on the downward slope.”
COVID-19: William Farr’s way out of the Pandemic
Great. Another Mission Accomplished: The spread of the virus has indeed slowed down. Not primarily due to any actions taken by either the authorities or the public, mind you, but because that’s how epidemics always behave, as William Farr observed in 1840. Why? Because, as biostatistician Knut Wittkowski explains in a paper first submitted to MedRxiv on March 28 and published on March 31,
“If a disease causes immunity after an infectious period of a few days only, like respiratory diseases, an epidemic extinguishes itself as the proportion of immune people increases.”
The first three months of the COVID-19 epidemic: Epidemiological evidence for two separate strains of SARS-CoV-2 viruses spreading and implications for prevention strategies
How does one become immune to a novel virus? By being exposed to it.
As the following model depicts, when a new virus enters a population, everyone is susceptible to becoming infected with it (blue line). As the virus moves from person to person, the number of infected people rises (orange line). After the virus’ incubation period (in the case of SARS-CoV-2, about 5 days), some of those infected people develop symptoms and are identified as cases (yellow line). Some of those cases succumb to the disease and die (grey area). All of the infected people who did not develop symptoms, and all of the cases who recover, are now resistant to the infection (green line). As the number of resistant people grows and the pool of susceptible people shrinks, the virus is unable to find enough susceptible people to infect, and hence the epidemic is extinguished.

Let’s now turn to a careful examination of the graph of case reports in Australia, annotated with the date of interventions. In the graph below, ‘cases’ include both people with symptoms (meaning that they may have been infected up to two weeks before being tested, given a roughly 5 day incubation period, a further period in which their symptoms worsened to the point where they sought medical attention, and a further 2 day delay before the test is processed and results are reported) and asymptomatic people who were tested because they were identified as actual or potential contacts of cases.
This makes it difficult to identify the peak of infections (i.e. the date on which transmission of the virus from person to person reached its highest point), but it most certainly preceded the peak in reported cases by at least several days. This means the peak of infections occurred before 15 March, and may have been as early as 10 March.
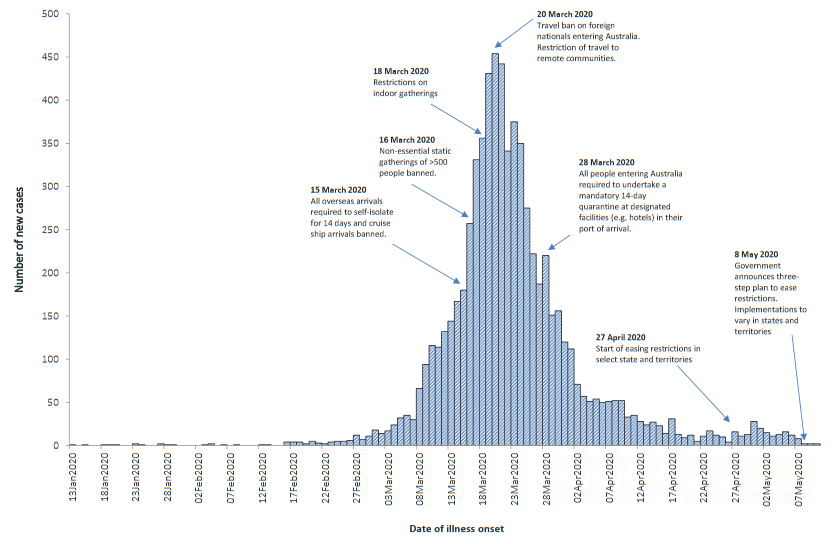
Interventions
15 March: overseas arrivals required to self-isolate for 14 days and cruise ship arrivals banned.
As already mentioned, the peak of infections occurred before this date and the peak of reported cases occurred just 5 days after it. Given that by the time the peak of cases occurs, the pool of susceptible people is already rapidly shrinking, this measure was of dubious effectiveness.
16 March: Non-essential static gatherings of >500 people banned.
Again, given the presumptive date of the peak of cases, and its relationship to the ratio of susceptible to resistant people, not to mention the general lack of evidence for efficacy of cancellation of most types of mass gatherings in limiting the spread of respiratory infections, this measure was of dubious effectiveness.
18 March 2020: Restrictions on indoor gatherings
Once again, since the peak of recorded cases occurred just two days after this measure was implemented and the peak of infection occurred at least 5 days earlier, its role in slowing down transmission of the virus is highly questionable.
20 March 2020: Travel ban on foreign nationals entering Australia
To reiterate, the peak of reported cases occurred on this date, rendering this measure largely ineffective. The World Health Organization (WHO) specifically recommends against border closures for mitigating the risk and impact of influenza epidemics:

There is no evidence that border closures (including the State border closures that occurred on 20 and 21 March) would be any more effective in containing the SARS-CoV-2 epidemic, which in any case hardly qualifies as a ‘severe pandemic’; the UK government downgraded its status on 19 March 2020:
“COVID-19 is no longer considered to be a high consequence infectious disease (HCID) in the UK… [largely because] more information is available about mortality rates (low overall).”
28 March: All people entering Australia required to undertake a mandatory 14-day quarantine at designated facilities (e.g. hotels) in their port of arrival
This is specifically “Not recommended in any circumstance” by the WHO even in the most severe influenza pandemics:

A quarantine implemented at an early point in an epidemic may delay transmission of the virus, but even the strict quarantine measures eventually instituted in China (over 1 month after the novel virus was identified) only succeeded in delaying “but did not prevent the global dissemination of SARS-CoV-2“.
Why a quarantine on overseas arrivals to Australia was implemented at a point when the SARS-CoV-2 epidemic was clearly on the decline is anyone’s guess.
The curve has been flattened, and the spread of the virus has slowed down. So why can’t we go back to work, school and our normal activities? Because now the objective of the War on SARS-CoV-2 appears to be to relentlessly track down every last case of the virus, through contact tracing.
Again, WHO specifically recommends against contact tracing as a response to influenza:

The same arguments against contact tracing apply in the case of SARS-CoV-2, especially on a population-wide basis at this late stage in the epidemic, given that the only valid function of contact tracing is to “collect information on the characteristics of the disease and to identify cases, or to delay widespread transmission in the very early stages of a pandemic in isolated communities”:

The fog of the war on COVID-19 has been generated by shifting and unclear objectives, lack of critical examination of the rationale for all the measures employed in prosecuting this war, and the consequent complete inability for anyone to determine when hostilities should cease.
In the final analysis, it was always a phoney war in any case. SARS-CoV-2 will do what viruses have always done – adapt by mutating into different forms, evolving new strategies to perpetuate itself by finding a new host species, decreasing its virulence in order to become endemic, or any combination of a myriad of other survival strategies – regardless of the puny efforts of hubristic humans. It, or its multiplicity of altered progeny, will still inhabit Earth long after we have managed to wipe ourselves off it.
We have met the enemy, and it is us.
Remember, taking good care of your health is even more important than usual due to the high levels of stress generated by the world’s response to COVID-19, and the fact that people with pre-existing chronic disease are at higher risk of serious complications of any type of infection, including SARS-CoV-2.



