2 April 2018; updated 5 September 2025
Over the 30 years that I’ve been in clinical practice, I’ve become increasingly disturbed by the creeping medicalisation of human suffering. Life, as the Buddha pithily put it, is suffering. All cultures, throughout human history (and presumably, prehistory), have simply accepted suffering as an inevitability, and have developed religious practices and philosophical teachings to help people come to terms with, make sense of, and ultimately to transcend, their suffering. All cultures, that is, until the mid-twentieth century in the secular West, when a series of chance discoveries led to the development of the first drug ever marketed as an antidepressant, iproniazid1.
The repackaging of ineluctable human suffering as ‘mental illness’ has accelerated at an ever-increasing rate since the accidental finding that launched iproniazid into a marketplace that was only too eager to accept a chemical fix for the travails of life.
A terrifyingly high percentage of my clients are either currently taking, or have taken in the past, psychiatric medications including antidepressants, anti-anxiety agents and atypical antipsychotics (disingenuously marketed as ‘mood stabilisers’).
Many have been on antidepressants for several decades, despite the fact that clinical trials for such drugs typically last for only eight to twelve weeks, and not a single clinical trial for any of the ten most-prescribed antidepressants has run for longer than one year. Just this week, I spoke to a client who has been taking antidepressants of various descriptions for 25 years, which amounts to almost two-fifths of her lifespan. And of course, many of my younger clients first started taking these powerful mind-altering chemicals in their teens, long before their brains had reached maturity.
I’ve written before about the complete absence of evidence for the ‘biochemical imbalance’ theory as well as the total lack of validity of diagnostic criteria for these so-called mental illnesses such as depression and anxiety.
However, despite the proliferation of books which provide meticulously-researched critiques of psychiatry and its arsenal of drugs, including Dr Peter Breggin’s many titles (start with Toxic Psychiatry, Talking Back to Prozac and The Antidepressant Fact Book), Robert Whitaker’s Anatomy of an Epidemic and Psychiatry Under the Influence; Gary Greenberg’s Manufacturing Depression; Dr Irving Kirsch’s The Emperor’s New Drugs; Dr Peter Gøtzsche’s Deadly Psychiatry and Organised Denial and Dr James Davies’ Cracked, many people are still being diagnosed with ‘illnesses’ that they don’t have, and prescribed ‘treatments’ that can’t possibly help them.
Antidepressants are now the most commonly prescribed class of drugs in Australia, and we denizens of the lucky country have the dubious distinction of having one of the highest rates of antidepressant prescription in the world. Roughly one in every seven Australians takes some form of antidepressant; that’s 3.9 million of us popping a pill that’s supposed to alleviate our mental suffering, every day.
As three psychiatry researchers recently pointed out in a trenchant opinion piece in the Medical Journal of Australia,
“It is unlikely that 14% of the Australian population would fit the clinical guideline criteria for antidepressant use. Clinical guidelines recommend non‐drug interventions as first line for anxiety and less severe depression, and ‘in severe major depression’ antidepressant therapy for ‘6 to 12 months, then consider deprescribing’.8 It is widely accepted that antidepressant effects ‘may be minimal or non‐existent, on average, in patients with mild or moderate symptoms’.9 A recent systematic review and network meta‐analysis ‘found some forms of exercise to have stronger effects than [selective serotonin reuptake inhibitors] alone’.10”
Antidepressant prescribing in Australian primary care: time to reevaluate
And yet, despite the wildly inappropriate overuse of these medications, there is a constant drum-beat in the media that ‘mental illness’ is underdiagnosed and undertreated, with a periodic cymbal-clash (usually triggered by a tragic mass shooting episode in the US) of calls for population screening for mental health conditions, especially in adolescents. Just last month, Illinois became the first US state to institute mandatory annual ‘mental health’ screenings for students in grades 3-12, commencing in 2027. And right on cue, a seriously disturbed individual who had obsessively studied the ‘careers’ of previous mass shooters for many years, opened fire on a Minnesota Catholic school church, killing two children and wounding 18 others and prompting a call to “expand… mental health infrastructure” in order to forestall a repetition of the tragic event.
The idea of population screening has a common-sense appeal to it. After all, surely it would be better to ‘catch’ a condition early in its development when it is easier to treat, rather than allowing it to fully develop? This is the logic behind cancer detection programs such as screening mammography and PSA testing… and unfortunately, neither works: screening mammography doesn’t save women from dying of breast cancer or reduce the death rate overall, and PSA testing doesn’t save men from dying of prostate cancer either.
In the case of depression, aside from the ineffectiveness of the mainstay of treatment, antidepressant drugs, the primary problem with population screening is the question of which screening tool to use.
Physical illnesses are diagnosed through objective signs and symptoms which can be observed and measured. Screening for hypertension or diabetes, for example, is quite simple – just measure people’s blood pressure or fasting blood glucose, and compare it to the cutpoints at which the risk for stroke, cardiovascular disease or diabetes begins to escalate2.
But since there are no biomarkers for psychological conditions such as depression and anxiety, the diagnosis of ‘mental illnesses’ is highly subjective. Consequently, various screening tools have been developed to allow clinicians to detect potential cases of depression and anxiety, with two of the most commonly used ones being the PHQ-9 Patient Health Questionnaire for depression, and the GAD-7 Generalised Anxiety Disorder Assessment.
GPs often have charts of these questionnaires in their consultation rooms. Even if you’re not seeing your doctor to discuss concerns with your psychological state, you’re liable to be handed one of these screening tools, before or during your appointment, just like this young woman:
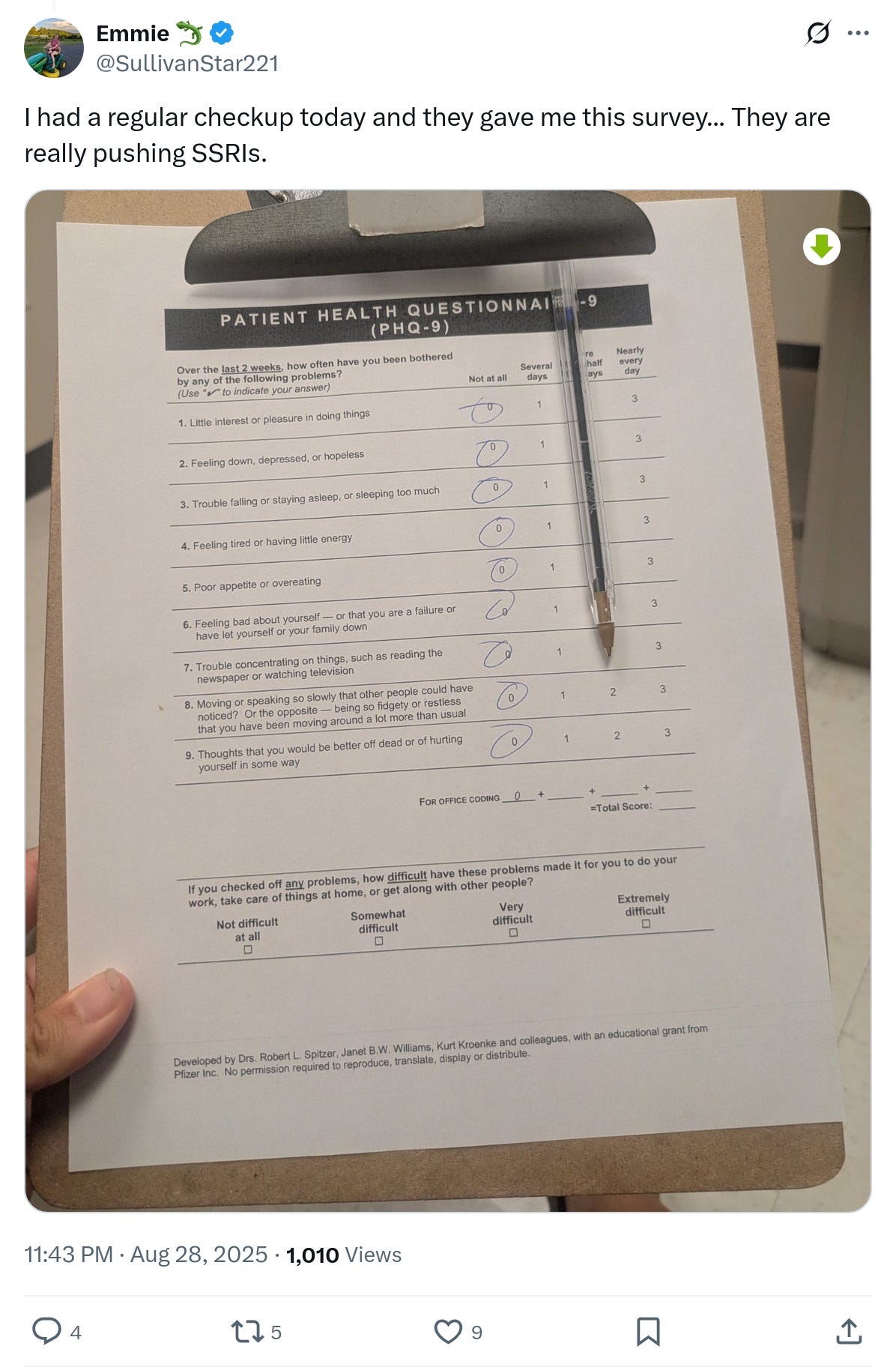
Many of my clients have told me that they were prescribed psychiatric medications on the basis of their responses to these questionnaires, even though they are not intended to be used as diagnostic tools.
Brought to you by Pfizer
None of these clients were aware that both screening questionnaires were developed by academics funded entirely by the pharmaceutical giant Pfizer, and that Pfizer owns the intellectual property and is responsible for distributing the PHQ-9 and GAD-7 to doctors.
Pfizer just happens to make some of the drugs most widely-prescribed for depression and anxiety, including venlafaxine (Efexor), sertraline (Zoloft), escitalopram (Lexapro) and alprazolam (Xanax).
Do you see the problem? It’s clearly in Pfizer’s financial interest to engage in disease-mongering – that is, expanding the diagnostic boundaries for a condition, to maximise the number of people who ‘qualify’ for diagnosis and treatment.
As Robert Whitaker has pointed out, pharmaceutical treatment of depression has actually turned it into a chronic condition that is far more likely to recur throughout an individual’s lifetime than in the pre-antidepressant era. So it makes perfect business sense for Pfizer to recruit ‘customers’ for their drugs, preferably at a young age, using busy GPs who aren’t adequately trained and resourced to talk to patients about their psychological issues, as their ‘pushers’.
It shouldn’t come as a surprise then, that the ability of the PHQ-9 to identify depression is low; it has a “positive predictive value of about 50%” which means that fully half the people that it identifies as potentially depressed are in fact suffering from some other health condition (or perhaps simply the human condition).
Pfizer also funded a GP training program dubbed SPHERE, which claimed to increase GPs’ competence at diagnosing and treating mental health conditions. The result was a significant boost in prescription rates of Pfizer’s flagship antidepressant, Zoloft. Did it improve patient care? Almost certainly not – a study conducted by Monash University researchers on the SPHERE screening tool found that its use would result in large numbers of psychologically healthy people being classified as having a probable mental illness. The authors wrote,
“As a global screen for mental disorder it had a very high false-positive rate, with, in one sample, 83% of patients screening positive while only 27% had a current psychiatric diagnosis, and in the other sample 55% screened positive with only 13% having a current psychiatric diagnosis.”
An examination of the efficiency of the 12-item SPHERE questionnaire as a screening instrument for common mental disorders in primary care
Big Pharma doesn’t restrict its activities to cultivating doctors. Drug companies also provide funding for not-for-profits, and they establish fake ‘grass roots’ organisations (known as ‘astroturfing’) to push their agenda to government and the public, via the ever-accommodating media.
For example, the non-profit mental illness advocacy group, the Mental Health Council of Australia, receives funding from multiple pharmaceutical companies, via the ‘Mental Health Australia/Pharma Collaboration’.
As an investigation published by The Australian in 2006 revealed,
“The so-called ‘Pharma Collaboration’, unreported in the Australian media, linked the Mental Health Council of Australia directly to global pharmaceutical giants Pfizer, Eli Lilly, Glaxo SmithKline, Bristol Myers Squibb, Lundbeck, Wyeth and Astra Zeneca.
It has been a good deal for the non-profit council, which promotes itself as Australia’s peak mental health group, providing 8 per cent of its total income. It also seems to have benefited the drug companies, which have a strong financial interest in selling medication to treat mental illness, especially the ‘new epidemic’ of depression.”
Mental health takes industry pills
Brainwashing Reeducating young people about depression
In 2004, the Mental Health Council was funded by Pfizer to write a report, which was duly publicised in the media, on young people and depression. The report argued that “young people were dismissive of depression, which was an illness that required professional treatment“. And by ‘professional treatment’, they – of course – meant antidepressant medications, whose efficacy and safety record in young people is particularly abysmal.
That dismissive attitude that the Mental Health Council bewailed, reflected the prevailing perspective of the time – that is, back in the early aughts, most young people still understood that not every form of human suffering is an ‘illness’. Sometimes, life just sucks. Your parents get divorced; your granny dies; your boyfriend cheats on you with your bestie; you flunk a course. And, quite predictably, you feel utterly miserable for a while, until – hopefully – good advice and appropriate support from loved ones helps you pull through.
Ah, those were the days! But predictably, Big Pharma set about curing youngsters of this wrongthink. And the Mental Health Council was more than happy to assist:
“A December 2004 council submission to the Federal Government calling for more investment in mental health was fully funded by Pfizer, Janssen-Cilag, Eli Lilly and Bristol Myers Squibb.”
Mental health takes industry pills
Twenty years on, and now every school has multiple ‘mental health days’ and awareness-raising campaigns, engineered to brainwash kids into believing that the emotional turmoil that is part and parcel of growing up, is actually ‘mental illness’.
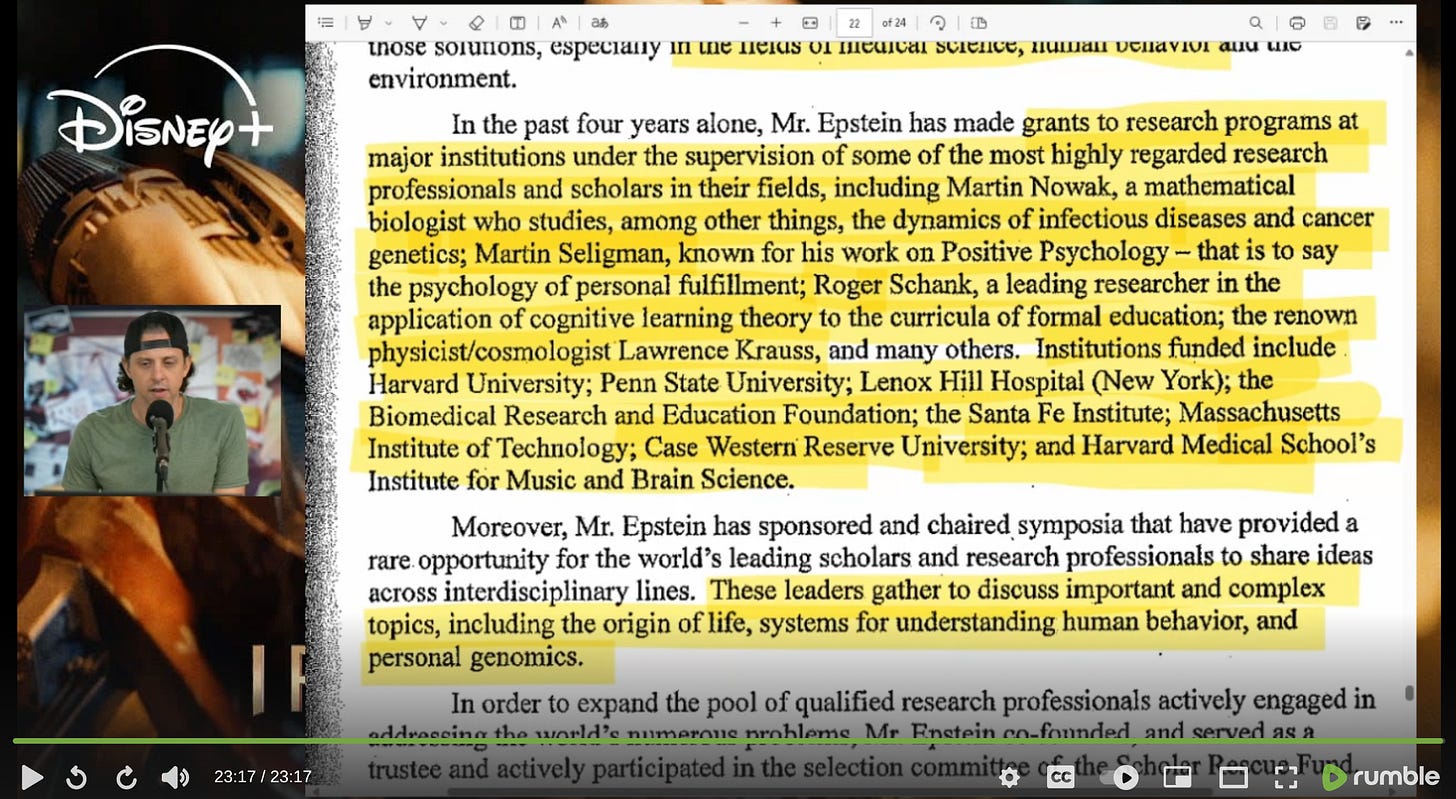
And here’s a darkly intriguing rabbit-hole: When my now-24-year-old son was in high school, all students were provided with school diaries that were structured around the positive psychology principles expounded by Dr Martin Seligman. Back then, I was an admirer of Seligman, having read several of his books. I had absolutely no clue that Seligman’s work had been financially backed since 2003 by Jeffrey Epstein – yes, that Jeffrey Epstein – when the mysteriously wealthy sex-trafficker-to-no-one stumped up the seed funding to create Seligman’s Positive Psychology Center at the University of Pennsylvania.
Seligman, whose ‘learned helplessness’ theory formed the basis of the brutal ‘enhanced interrogation’ – that is, torture – protocols deployed by the CIA and Pentagon on suspected 9/11 terrorists, helped Epstein to obtain the sweetheart prison deal in 2008, under which Epstein was permitted to serve an insanely lenient sentence for solicitation of prostitution with underage girls. After Epstein’s release from prison, Seligman obtained a US$31 million no-bid contract by the US military, to help develop soldiers’ ‘psychological resilience’.
Put bluntly, Seligman was tasked with developing methods for overcoming the inherent resistance to taking the lives of other human beings that exists in all healthy people, by psychologically engineering them into redefining killing as a virtuous act so that they could slaughter both combatants and civilians without developing posttraumatic stress disorder (PTSD). (Seligman’s program doesn’t actually appear to work, and US veterans are still suffering from sky-high rates of PTSD, resulting in an alarming incidence of suicide.)
How comfortable do you feel with this man’s work being incorporated into your child’s school curriculum?
While schools have played an important role in transforming young people’s attitudes about so-called mental illness, their impact has been eclipsed by that of the social media platforms. Tiktok, Instagram and Snapchat are deluged by content produced by young influencers, which incites their impressionable followers to misconstrue every episode of the blues as ‘depression’, every attack of nerves as ‘anxiety disorder’, and every instance of impaired concentration or disorganisation as ‘ADHD’… all of which require medication, naturally. Mission accomplished.
The obstacle is the way
Let’s be clear: psychological suffering is real. People do feel anxious, hopeless and unable to enjoy life. There are usually very obvious reasons why they feel that way – they’re lonely, they’ve suffered a significant loss, they experienced childhood trauma, or they’re stuck in a job, relationship or living situation that thwarts their human development. Sometimes they have a physical condition, such as a thyroid disorder, that is causing or exacerbating their psychological suffering.
Prescribing psychiatric medications never addresses the cause of a person’s misery; it simply casts them in the role of a helpless victim of aberrant brain chemistry. Even worse, antidepressants cause emotional blunting and impair reinforcement learning, which undermines our ability to learn from our environment so that we can change the behaviours and circumstances that are making us depressed or anxious.
And, contrary to the assertion that psychiatry and its diagnoses ‘relieve the stigma of mental illness’, they in fact cause suffering people to be stigmatised, as James Davies has pointed out – people are far more likely to be stigmatised when the cause of their aberrant behaviour is believed to be biological rather than social or psychological.
The bottom line: Screening tools and diagnostic criteria that are set by individuals or corporations with a vested interest in expanding diagnostic boundaries are not to be trusted. If you’re experiencing persistent anxiety, sadness, sleeplessness or oversleeping, loss of interest in activities that you formerly found enjoyable, overwhelming guilt or hopelessness, or a sense of disconnection from others, you should definitely seek help. But that help must address the reasons why you’re feeling the way you do, not just put you in a pharmaceutical straitjacket that blunts your capacity to experience any of your emotions – emotions with which you are equipped for the purpose of guiding you toward a richer, more fulfilling life.
Struggling with anxiety or depression? Apply for a Roadmap to Optimal Health Consultation today to find out how I can help.
- Gary Greenberg provides a gripping account of the development of iproniazid, and the other early antidepressants, in his highly readable book Manufacturing Depression. ↩︎
- It’s important to acknowledge that the role that both financial and non-financial conflicts of interest play in the formulation of these guidelines, and the consequent risk of overdiagnosis and overtreatment, is hotly debated. ↩︎




5 replies to "Who says you’re depressed or anxious? Pfizer does."
* Manufacturers influence our culture such that they create an analogy of a fish feeding frenzy. This is done through portraying the product to be associated with health, status, pride and socially a necessity.
* Humans are manipulated and milked for their money just like the cows are milked for their milk.
Thanks Robyn, good read.
I think the Black Dog Institute website is a very reputable resource for people.
https://www.blackdoginstitute.org.au
The Black Dog Institute uses the PHQ-9 as as their depression self-test (see https://www.blackdoginstitute.org.au/clinical-resources/depression/depression-self-test), without identifying it as such or disclosing the fact that the test was developed by Pfizer. Given the lack of specificity and sensitivity of this screening tool, it’s likely that the Black Dog Institute’s endorsement of it is likely to lead to overdiagnosis and overtreatment.
This is an interesting article. I work with young people who, due to past (and continuous) drug or alcohol abuse are one several antidepressants and anti-anxiety medication. A lot could be done for them if only there was a root cause investigation into their suffering. They eat poorly, don’t exercise, still consume drugs and alcohol from time to time. I have no ideea how to help them.
This is an incredibly challenging population to work with as they need such a comprehensive approach in order to get them back on track. Check out Adam Sud who was able to overcome drug addiction, food addiction, multiple psychological diagnoses and type 2 diabetes, and now runs a coaching program to help people like him: https://www.adamsud.com/