4 July 2022
In Part 1 of this series, I summarised the four major ways in which COVID-19 injections have interfered with the complex interactions between SARS-CoV-2 and the human immune system, then zoomed in on the first problem: the narrow and short-lived immune response that they generate.
In Part 2 I laid out the evidence that the injections are causing people to become susceptible to repeated infection, most likely through the mechanism of ‘original antigenic sin’, otherwise known as the Hoskins effect and immune imprinting.
And now, in Part 3, I’m going to focus on the consequences to individuals of the inability to clear viral infection that results from a limited and fixated immune response to SARS-CoV-2.
Problem #3. An ineffective immune response leads to high viral load and favours viral dissemination
It stands to reason that if a person isn’t able to generate a very effective immune response against a virus, the virus will be able to replicate freely in the person’s cells resulting in a high viral load. Here’s why:
The initial response to viral infection is handled by the innate immune system, which releases chemicals such as interferons that set in motion a whole suite of antiviral activities, as well as prodding the acquired immune system to initiate the process of developing immunological memory.
The acquired immune system produces antibodies and activated T cells which mop up any remaining infection, and ensure a speedier and more targeted immune response to any subsequent attempt by the virus to establish infection.
In a person with a normally-functioning immune system, the innate immune response results in the viral replication phase of COVID-19 peaking 3-4 days after infection and then rapidly declining such that the RNA copy number is below an infectious level by day 10.
However, because COVID-19 injections suppress the innate immune system’s response to viruses by a number of mechanisms including profoundly impairing type 1 interferon signalling, they permit much more viral replication than occurs in unjabbed people with an intact immune system. And because they fixate the acquired immune response on the now-extinct Wuhan variant of SARS-CoV-2, they hinder the development of immunological memory, permitting prolonged infection and reinfection.
The consequences of this interference with normal immune activity are evident in populations with high rates of COVID-19 injection (including high uptake of one or more booster shots), such as Israel and Portugal, which are seeing surging (and completely unseasonal) rates of serious illness, hospitalisation and death attributed to the BA.5 Omicron variant.
Israel’s “coronavirus czar” (an interesting title, given that a “czar” is an unelected autocratic ruler) Professor Salman Zarka was quoted as saying that “the new variant BA.5 is quickly gaining traction and is more resistant to vaccines than previous strains.”
“The strain caused relatively mild illness among young people, but we can see a rise in hospitalizations.”
Prof Salman Zarka, Israel sees 70% spike in number of seriously ill COVID patients within a week
In other words, the BA.5 strain has evolved to infect those who have taken one or more COVID injections more efficiently, and while most people will only experience a common cold-like illness from this infection, hospitals are seeing a rise in serious cases.
Why? Because BA.5 (and its close cousin, BA.4), appear to replicate very efficiently in human lung tissue, unlike the ‘original’ versions of Omicron which replicated like crazy in the mouth, nose and upper airway, but not in the lungs.
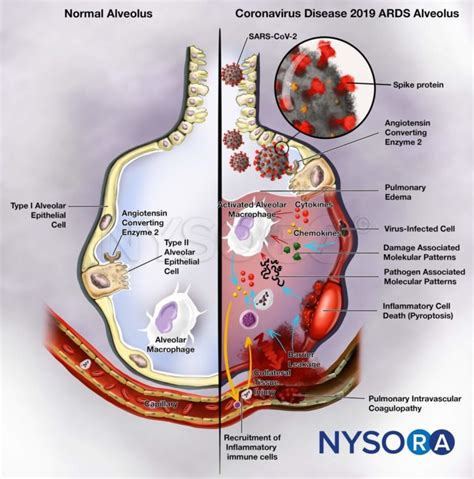
Under normal circumstances, if you have a high viral load in your nose, mouth and bronchus, you can expect common cold symptoms such as a headache, stuffy or runny nose, sore throat and cough. These symptoms are caused not by the virus itself but by the immune response to infection. A vigorous innate immune response results in production of inflammatory chemicals that destroy the virus-infected upper airway cells. It’s unpleasant, but not life-threatening.
But if a virus manages to replicate efficiently in your lungs, and your immune system destroys large numbers of virus-infected epithelial cells (the cells that line the lungs), gaps start to form in that lining. Large numbers of viral particles can slip through those gaps and enter the blood vessels that line the airways, and from there, they can infect other organs.
As noted in Why COVID-19 “vaccines” will never end the pandemic, COVID-19 injections cannot possibly prevent you from getting infected with SARS-CoV-2, because they don’t stimulate the production of secretory IgA which neutralises viruses at the mucosal level; the antibodies produced in response to the injections are confined to the bloodstream.
So the only justification for using these injections at all would be for the prevention of severe disease by stimulating the production of neutralising antibodies.
But as discussed in Part 2 (and further confirmed here), the antibodies stimulated by COVID-19 injections don’t effectively neutralise the Omicron variant, because they were made to ‘match’ the original Wuhan strain of the virus, which is now completely extinct. This impaired neutralising capacity allows the virus to travel through the bloodstream unhindered, and to infect cells in other organs (viral dissemination).
An autopsy study conducted in the pre-Omicron era (January to November 2021) found that people who had died of COVID-19 after receiving either one or two injections had more viral dissemination than people who were uninjected.
Only 16 per cent of the uninjected deceased had detectable SARS-CoV-2 outside of their upper airways and lungs, compared to 38 per cent of the double-jabbed and 69 per cent of the single-jabbed. Organs which were found to have been infected by the virus included the heart, kidney, pancreas, spleen and pituitary gland:
“A high rate of viral dissemination detected by RT-qPCR within the organ system was an unanticipated result in this study, which was especially accentuated in the partially vaccinated compared to fully vaccinated cases (11 of 16 vs. five of 13, respectively; P = 0.144). In several cases, RT-qPCR identified the RNA of SARS-CoV-2 in all investigated samples, including cerebrospinal fluid, CNS, and soft tissues. This is in strong contrast to a previously published collection of the Augsburg series of nonvaccinated lethal SARS-CoV-2 infections, in which the frequency of viral dissemination was rare, with a rate of only 16% (three of 19)17 instead of 69%.”
High viral loads: what drives fatal cases of COVID-19 in vaccinees? – an autopsy study
RT-PCR tests on the nasopharynx and lung tissue of injected people who had died of COVID-19 found low cycle thresholds, indicating a high viral load of SARS-CoV-2. All but two of the deceased individuals for whom serology was available had anti-spike antibodies, underlining the lack of protection against infection and viral replication in the airways that these antibodies confer.
A strong correlation was found between the absence of antibodies to the nucleocapsid protein of SARS-CoV-2 – which, as discussed in Part 1, is inhibited by COVID-19 injections – and the degree of viral dissemination. Nucleocapsid antibody appears to be critical to stopping the virus from spreading throughout the body, so the fact that injections retard development of these antibodies is deeply concerning.
The authors of the study noted the vitally important role of autopsies in understanding the pathophysiology of disease, and indicated their dismay that “reports on autopsies of SARS-CoV-2 breakthrough infections are widely lacking”. Given the rather damning findings of their own study, the dearth of autopsy reports on fatal outcomes of breakthrough infections are perhaps not too surprising.
As mentioned, the autopsy study covered deaths that occurred before the emergence of the Omicron variant. Omicron is an immune escape variant – that is, it has acquired mutations that render it resistant to the immune response engendered by COVID-19 injections.
While it was initially welcomed as a variant with low pathogenicity (disease-causing potential), as mentioned above, its subvariants BA.4 and 5 appear to have reacquired the tropism for (capacity to infect) the lung that the original Omicron had lost. Let’s consider why this might happen.
In a person with an intact immune response, the innate immune system would quickly bring a variant like the original Omicron, which was good at infecting the upper airways but lousy at infecting the lung, under complete control. The result: a common cold-like illness that lasts less than a week and generates enhanced mucosal immunity which is protective against subsequent symptomatic infection.
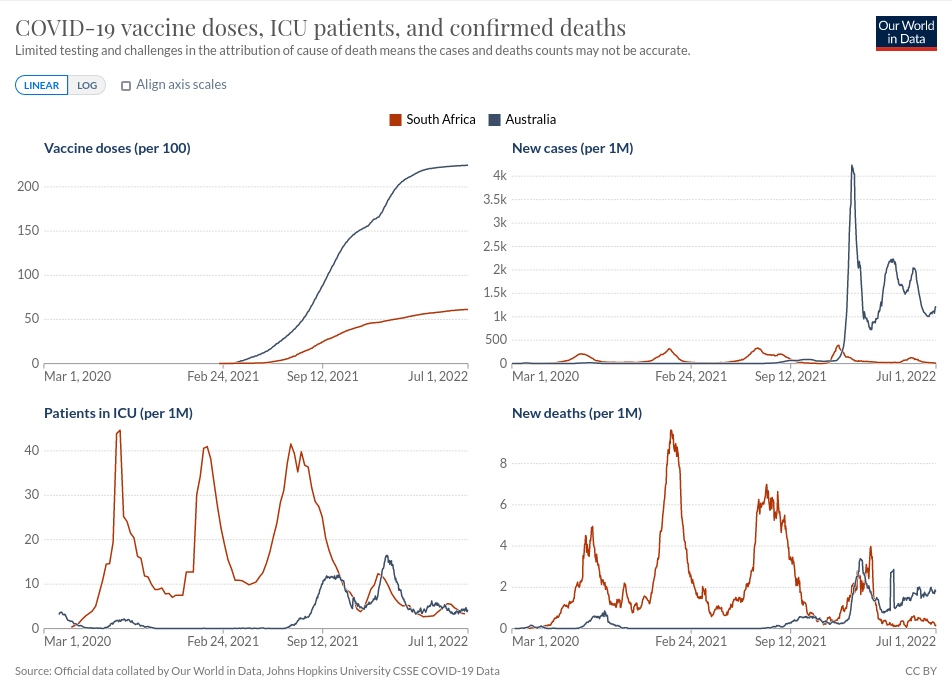
This is the experience that largely uninjected populations, such as South Africa, have had with Omicron; a spike of ‘cases’ that subsided quickly, resulting in fewer deaths than in all previous waves, and was succeeded by a downturn in the death rate.
In contrast, heavily-injected Australia has suffered several mortality spikes since the supposedly mild Omicron variant attained dominance, and the death rate continues to tick up inexorably.
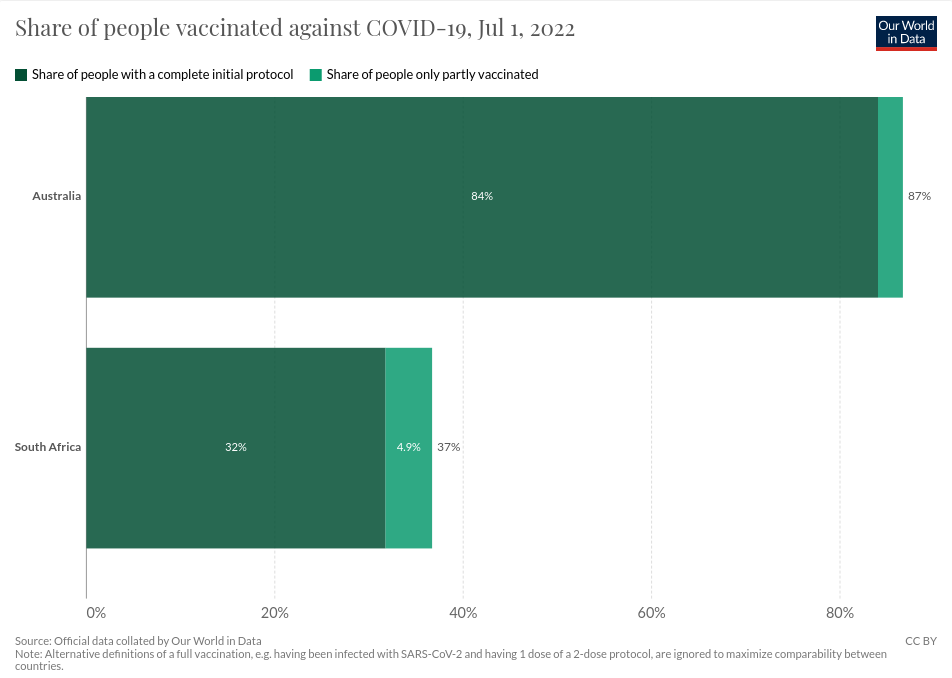
First let’s look at a comparison of injection rates between the two countries:
And now the outcome data:
What we are experiencing in Australia is precisely what we would expect to see, given what we know about the impact of these experimental injections on the immune system:
- An impaired innate immune response prevents the clearance of the Omicron variant from the upper respiratory tract.
- The virus replicates freely, and as it does so, its progeny spontaneously develop many mutations in their genetic code.
- While most of these mutants don’t survive, some, by sheer chance, develop tropism for the lung (BA.4 and 5).
- They begin to replicate in the lungs, and from there, disseminate throughout the body because they are not neutralised by injection-induced antibodies, allowing them to infect organs and cause potentially fatal damage.
People who already have an impaired innate immune response – such as the elderly and those with comorbidities like obesity, diabetes and heart disease – are most at risk, but even young, formerly healthy people may succumb.
And in the mean time, due to their high viral load, they are exhaling large numbers of viral particles with high contagiousness and tropism for the lung. We’ll explore the consequences of that in Part 4.



