From the moment that DMSO’s star began to rise, in December 1963, its status as a potential wonder-drug rested on claims that it relieved the diabolical duo of pain and inflammation. The first wave of DMSO-hyping newspaper and magazine articles published in 1963 and 1964 (discussed in Part 2 of this series) focused on Dr Stanley Jacob’s success in using it to treat arthritis, burns, injuries, and other assorted painful and/or inflammatory conditions.
In that era, American medicine was a far more decentralised business than it is now. Most doctors worked in solo or small group practices rather than as employees of large healthcare systems, and while clinical practice guidelines were beginning to appear, doctors still had a degree of professional autonomy with respect to choosing treatments for their patients, that today’s primary care providers would find astonishing. Hence, when DMSO came to public attention via the popular media – and, subsequently, after Jacobs published his first two scientific papers on the universal-solvent-cum-wonder-drug – doctors across America began trying it out on their patients.
This mass-scale experimentation produced a slew of papers in medical journals, in which Jacob and other doctors described the results they had observed in patients they had treated for musculoskeletal injuries such as strains, sprains, bruises and contusions, and inflammatory conditions of the musculoskeletal system such as bursitis, tendinitis and arthritis. These early papers (e.g. see here, here, here, here, here and here) described many cases of dramatic reductions in pain and swelling, and equally dramatic improvements in recovery time, range of joint movement, and general function. They also documented many partial and complete failures.
The general consensus that emerged over time was that DMSO was highly effective for pain relief and speeding up healing in most acute conditions – that is, those with sudden and severe onset such as sprains, strains and sports injuries – but less reliable for chronic conditions such as osteoarthritis and rheumatoid arthritis, especially in joints with longstanding inflammatory involvement.
As intriguing as these early reports are to read, they suffer from three major limitations:
1. Cursory descriptions of cases
The descriptions of patients’ responses to DMSO treatment (when there are descriptions of individual patients’ responses; many of them are simply summaries that rate patients’ responses in some arbitrary fashion, such as ‘improved’ or ‘unsatisfactory’) read more like rather entertaining stories or the types of testimonials one might find on an internet sales pages, than formal case reports. No doubt this is a reflection of the standards of medical journals at the time, but for modern readers who are accustomed to reading contemporary case studies and case series, the lack of detail is disconcerting. There is little to no diagnostic information provided, little to no individual-level description of previous treatments and their outcomes, and little to no documentation of follow-up. The reader is simply expected to take the doctor’s word for it that the cases presented and unfolded as described.
2. No standardisation of pain or function ratings
Numerous clinical instruments have been developed to quantify key features of musculoskeletal conditions, such as pain, stiffness, disability and physical function. The most widely-used such instrument in studies on musculoskeletal conditions is the Western Ontario and McMaster Universities Arthritis Index (WOMAC), which was first presented in 1988. These instruments allow clinicians and researchers to evaluate the effects of treatment protocols with a high degree of reliability and validity, or in lay terms, consistent and accurate measurement.
Obviously, it’s unfair to criticise Stanley Jacob and other early proponents of DMSO for not using a clinical instrument that hadn’t even been developed yet! Nonetheless, comparison of the early reports of use with later trials that used WOMAC to rate outcomes, is telling; DMSO failed to beat out placebo for pain relief in osteoarthritis and was inferior to diclofenac for physical function, stiffness and pain on walking.
3. No control condition
Case studies and case series aren’t expected to have a control condition (i.e. a random allocation of patients to receive either DMSO, or an inactive placebo, and/or a standard, established treatment); they are used in the medical literature to educate clinicians about rare diseases that might occasionally be seen in practice, to suggest novel treatment approaches, or to bring attention to adverse reactions that might otherwise be missed. But a case series typically comprises ten or fewer patients; when one is reporting [in a very cursory fashion, it should be noted] on results gained from treating over 500 patients, not using any type of control condition is highly questionable.
Stanley Jacob and colleagues attempted to address the lack of a control condition in one of their DMSO reports, as follows:
“The criticism sometimes made that clinical trials reported here for dimethyl sulfoxide lack comparison with control studies can be answered. Except for a few instances, all patients had received or tried other remedial measures such as heat, salicylates, methyl salicylate, liniments, ointments, and in a number of patients, oral phenylbutazone and corticosteroids, or injections of corticosteroids without significant benefit before trial with DMSO. At the beginning of this study ten patients with acute subacromial bursitis first had their shoulders painted with a solution of glycerol and were observed for 30 minutes; in none was there any relief of pain or increase in motion noted from the placebo. The area was then wiped dry and DMSO applied with, in most cases, noticeable benefit reported by the patient.”
‘Dimethyl Sulfoxide in Musculoskeletal Disorders‘
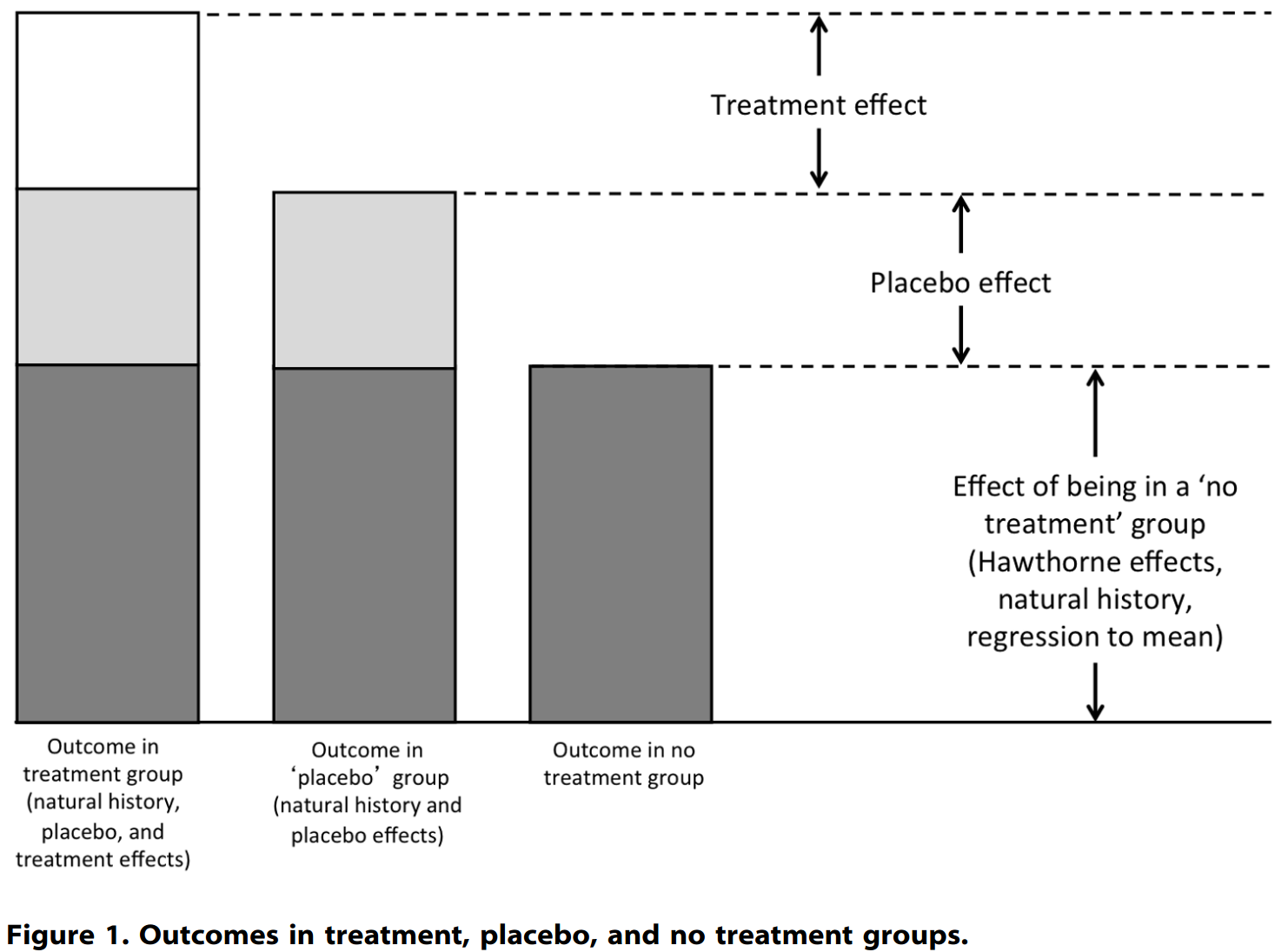
I don’t find this to be a compelling rationale for the lack of a control group, for two reasons: firstly, the placebo effect; and secondly, the natural history of disease, a set of other variables commonly conflated with the placebo effect.
The placebo effect
It has long been observed that novel treatments seem to ‘work’ better than established treatments; an 18th century French physician is reported to have quipped to a patient,
“Prenez, madame, et dépêchez-vous pendant qu’elle guérit. (Take it, madame, and hurry up while it [still] cures.)”
Michel-Philippe Bouvart
The observation that patient expectations have a profound impact on clinical outcomes gave rise to the study of the placebo effect, or placebo response, which I discussed at length in The placebo paradox. Placebo responses are “genuine psychobiological events attributable to the overall therapeutic contex“, and pain is one of the features of illness that is most susceptible to their impact. Furthermore, the magnitude of impact of the placebo response on patient outcomes “may be greater for novel interventions and for procedures“. The attitude of the treating physician toward the intervention also has a profound effect on patient outcomes, whether or not this attitude is made explicit to the patient:
“Clinicians who strongly advocate a new procedure for a disease often have significantly positive results… More subtle clinician biases have also produced clinical changes in controlled studies (Levine and Gordon, 1984; Gracely et al., 1985).”
‘Placebo effects: clinical aspects and neurobiology‘
Let’s put this all together: Patients with various painful and disabling conditions, many of which had not responded adequately to previous treatments, were given a novel treatment that had been hyped in prestigious national news media… and to top it all off, many were treated by (or at least, under the supervision of) the great Dr Stanley Jacob himself, who by this time had become famous thanks to being featured in those media articles. You could not get a better set-up for a placebo response.
Finally, the argument that designing a placebo-controlled trial for DMSO is next to impossible because of the distinctive garlic breath, garlicky body odour and skin irritation that it generates, is invalidated by the use in many studies of a 10 per cent DMSO solution as the control condition. At this low concentration, topical DMSO has little or no therapeutic effects but does still produce the characteristic breath odour and even skin irritation generated by higher, and supposedly therapeutic, doses.
Natural history of disease
In any given illness or condition, there is tremendous variability in the symptoms experienced by the same individual at different points in the course of the illness, and in symptoms experienced by different patients with the same illness. These variables – the natural course of disease, fluctuations in symptoms, regression to the mean (the statistical phenomenon by which extreme variables tend to be closer to the average the next time they’re measured), as well as response bias with respect to patient self-reporting of
subjective symptoms – are often ‘lumped in’ with the placebo effect, but in fact they represent the inherent tendency of conditions and illnesses to either go away without any treatment at all, or to fluctuate over time:
Especially when dealing with acute musculoskeletal conditions, most of which spontaneously resolve with no treatment at all, the failure to include a control group is a major red flag. Here’s a telling comment by the authors of a review of over 1900 patients treated with DMSO for various musculoskeletal disorders:
“Beneficial results are unpredictable, but they occur frequently and are sometimes dramatic, particularly in acute conditions, which require low doses and short treatment periods.”
‘Dimethyl sulfoxide in musculoskeletal disorders‘
… which a sceptic might translate as, in people who were almost certain to get better anyway, it sure looked like DMSO made them get better faster. Cool story, bro. Personally, I’d want to see evidence a bit harder than that, before I jumped on the DMSO bandwagon.
Likewise, in a 1981 Sports Illustrated article on attitudes of athletes, trainers and physicians to the use of DMSO in sports, distance runner Alberto Salazar mused,
“It is fickle stuff. Sometimes I get immediate relief and other times it doesn’t seem to work at all on a similar problem. It’s mysterious.”
‘A miracle! Or is it a mirage?‘
Nonetheless, multiple studies have been conducted, both in vitro (literally ‘in glass’, meaning, conducted outside the living body) and in laboratory animals, which reveal multiple mechanisms via which DMSO dampens inflammation and relieves pain. That may sound absolutely wonderful to you if you’re suffering from a painful, inflamed condition. But two major caveats apply to these mechanistic studies: Firstly, cells removed from the body and studied in culture do not behave as cells do in a living body; and effects observed in animals often don’t replicate in humans. And secondly, acute pain has a purpose, and inflammation is the second stage of healing (after haemostasis, or actions to control blood loss); hence, it’s not always a good idea to suppress either of them. A thorough understanding of the mechanisms by which DMSO reduces pain and inflammation is vital in order to decide whether to use it in any given circumstance. These mechanisms include:
1. Antioxidant activity
At low concentrations, DMSO has antioxidant activities, acting as a scavenger of free radicals – that is, molecules with an unpaired electron, that seek to ‘steal’ an electron from any nearby molecule. Free radicals cause oxidative stress within cells. DMSO has a particular affinity for hydroxyl radicals, highly reactive species that, if not quenched by antioxidants, causes irreversible damage to proteins, cell membranes and DNA, contributing to chronic disease and aging.
In human endothelial cells extracted from the umbilical vein, DMSO was found to ‘switch on’ a protein called nuclear factor erythroid 2-related factor 2 (Nrf-2). Nrf-2 is a master regulator’ of the body’s response to oxidative stress. Cellular stress generated by oxidative damage from inflammation or injury activates Nrf-2, which then turns on a number of genes that produce a whole range of antioxidant enzymes and detoxifying proteins including catalase, superoxide dismutase and glutathione. In other words, at least in a petri dish, DMSO activates the body’s own defence mechanisms against oxidative stress.
On the other hand, at higher concentrations, DMSO may act as a pro-oxidant by participating in the formation of the superoxide radical anion. DMSO failed to prevent gastric lesions induced by oxygen-derived free radicals in rats. In rat brains, DMSO protected against lipid peroxidation by some pro-oxidants, but increased oxidative damage to proteins. And in a rabbit model of antigen-induced arthritis, secondary cartilage loss and x-ray-detected erosions were worse in the group treated with topical DMSO.
2. Anti-inflammatory activity
In in vitro studies, DMSO suppressed the release of free radicals from human neutrophils. Neutrophils are the first immune cells to respond to tissue injury or infection. They fight bacteria and other microbes by releasing reactive oxygen species including superoxide and hydrogen peroxide; these compounds also trigger acute inflammation, causing tissue damage.
However, neutrophils are also vital for tissue repair and regeneration after infection and injury. The reactive oxygen species that they release initiate angiogenesis, the formation of new blood vessels necessary for wound healing and regrowth of tissue. While excessive reactive oxygen species cause ongoing tissue damage that inhibits healing, total suppression of reactive oxygen species release by neutrophils also interferes with tissue repair. Neutrophil activity is absolutely critical to the healing of skin, muscle (including heart muscle), bone and liver, among others.
In vitro, DMSO was found to inhibit the ability of neutrophils to kill Staphylococcus aureus, a skin bacterium that can cause boils, abscesses, cellulitis, pneumonia and heart valve infections. And in rabbits who were injected with DMSO, and then had Staphylococcus aureus injected into their lungs, significantly fewer neutrophils migrated into the lungs compared with rabbits who only received the Staph injection (controls). Thanks to their freely-migrating neutrophils, control rabbits were able to clear the Staph bacteria from their lung fluid in under 24 hours, while rabbits injected with DMSO still had Staph hanging around after 72 hours. Finally researchers who inflicted burns and scalds on rats and rabbits (seriously, wtf is wrong with these people????) found that neither topical application of 50 per cent DMSO to the burn site, nor application of 70 per cent DMSO to a distant, shaved site, reduced inflammation, oedema (swelling) or healing time.
What are we to make of all this? The practical implication is that using DMSO for acute wounds and injuries may backfire. The price you pay for pain relief and reduced inflammation, may be increased risk of infection, and delayed and incomplete healing, which could increase the risk of future injuries. There is credible evidence that nonsteroidal anti-inflammatory drugs (NSAIDs) may negatively affect the healing process in several types of musculoskeletal injury, and that NSAID use does not slow down joint deterioration in osteoarthritis. Only randomised controlled trials with adequate follow-up periods, and diagnostic procedures to assess healing rates and tissue quality, will provide definitive answers to the question, Will DMSO make me feel better in the short term, while making me weaker and more injury-prone in the long term?
3. Blocking pain signalling
DMSO impedes conduction in C-type nerve fibres, which mediate some of the sensations that our brain interprets as pain. In experiments conducted on cats, concentrations of DMSO as low as 5-7 per cent were found to slow down C fibre conduction, while concentrations of 9 per cent and above blocked it completely.
C fibres are unmyelinated, slow-conducting fibres that react to “high-intensity mechanical, chemical and thermal stimulation” such as crush injuries, sprains and strains, touching extremely hot or cold objects, and physiological changes such as low blood sugar and accumulation of muscle metabolic products. The type of pain carried by C fibres is diffuse (i.e. hard to pin down to one specific location), aching or sore rather than sharp or pricking, and often described as “annoying and intolerable”.
When nerves are damaged or repeatedly subjected to noxious stimuli, C fibres produce central sensitisation, or sensitisation in the spinal cord, which leads to hyperalgaesia (abnormally increased sensitivity to pain) and allodynia (pain responses from previously non-noxious stimuli, such as light touch). The burning pain that often persists for months after an attack of shingles, known as postherpetic neuralgia, and complex regional pain syndrome (CRPS) are two examples of central sensitisation. CRPS (formerly known as acute reflex sympathetic dystrophy) is a chronic pain condition that affects one limb or extremity, usually after an injury. It is believed to be caused by damage to, or malfunction of, the peripheral and central nervous systems, leading to an over-protective pain system. Aside from pain, CRPS sufferers experience changes in skin colour, temperature, and/or swelling and sweating.
Evidence that DMSO (in combination with idoxuridine, an antiviral drug) relieves postherpetic neuralgia is limited, as has been adoption of this treatment option. And while a multidisciplinary Dutch CRPS task force rated 50 per cent DMSO cream as effective for CRPS type 1, especially the ‘warm’ type, assigning it a level 2 evidence standard, a more recent Cochrane review described the evidence for benefits of DMSO as generally poor quality, concluding that “topical DMSO may not reduce pain intensity” in CRPS.
DMSO’s effect on collagen – cause for concern
In both animal experiments and in human patients with scleroderma, repeated topical use of DMSO was found to accelerate breakdown of collagen and to weaken its structure, while in chick cell lines, it inhibited collagen production. This is a useful therapeutic effect in the case of scleroderma, a condition which involves excessive collagen production which leads to hardening, thickening and tightening of the skin and other organs, but in the animal experiments it resulted in decreased strength of skin and tendons. In rats, cuts in the skin initially appeared to close up faster when DMSO was applied to the wound site, but after three weeks, control rats’ wounds had healed far more completely than the DMSO-treated rats. Researchers noted differences in the type of collagen fibres produced in rats treated with DMSO that may have accounted for the delayed wound healing.
What does it all mean????
If you’ve made it this far, congratulations! You’re clearly a person who is interested in gaining deep understanding of a topic, and can tolerate ambiguity. These two qualities are vital in insulating you from the very human tendency to jump on any bandwagon that happens to be rolling past. And boy, is DMSO a grade-A bandwagon!
Nonetheless, you might be feeling rather frustrated if you read this article to answer the question, Should I use DMSO for my condition or injury?
My honest answer is,I don’t know. The quality of the research on DMSO (and, dear reader, I ploughed through an ungodly number of papers to write this post) is far from impressive. The level of certainty for any of the claimed benefits of DMSO is so low, it’s virtually subterranean. And DMSO does have adverse effects – some of them pretty serious, as I’ll discuss in a later part of this series. If you do decide to experiment with using DMSO, here are two quotes to keep in mind. The first is from Dr Stephen Edelson, who was quoted in a 1996 article titled ‘DMSO: Many Uses, Much Controversy’. Edelson reported making extensive use of DMSO for “all sorts of inflammatory conditions, from people with rheumatoid arthritis to people with chronic low back inflammatory-type symptoms, silicon immune toxicity syndromes, any kind of autoimmune process.” Despite his enthusiasm for its use, Edelson stressed,
“DMSO is not a cure… It is a symptomatic approach used while you try to figure out why the individual has the process going on.”
‘DMSO: Many Uses, Much Controversy‘
And, in the Sports Illustrated article cited above, veterinarian Joe Burch, who was familiar with the use of DMSO in race horses, emphasised:
“We don’t know all about its workings yet, but that one’s for sure. DMSO doesn’t heal tissue. The body does that for itself. DMSO just makes it easier, quicker and pain-free.”
‘A miracle! Or is it a mirage?‘
The body heals itself. The symptoms of inflammation – pain, swelling, redness, warmth and loss of function – are actually signs that the body is actively engaged in healing itself. That healing process can be disrupted by the presence of factors inimical to healing, and the absence of factors required for healing. If you wish to facilitate healing, your first step should be to optimise every one of these factors, by eating a minimally-processed plant-forward diet, adopting a movement program that’s suitable for your current condition, ensuring you’re getting enough good quality rest and sleep, getting outdoors into natural light, and meeting your need for healthy human connection.
In the next instalment, I’ll be exploring the use of DMSO for a very particular type of pain – namely, cancer pain – and the contradictory evidence regarding DMSO’s effect on cancer itself.



