Fat chance of getting healthy on an ultra-low carb diet
27 October 2025
A reader’s response to What has happened to our doctors? prompted me to indulge in a mini-rant about the dangers of doctors with minimal training in nutrition, jumping on the bandwagon of promoting diet trends like ‘keto’, because they lack the foundational knowledge of the impact of dietary patterns on human health over the long term:
And, right on cue, a new study popped onto my radar, which examined the effects of long-term adherence to a ketogenic diet on body weight, liver fat, blood glucose regulation, insulin secretion and other markers of metabolic health. Spoiler alert: it’s not good news.
I will acknowledge the principal limitation of this study up front: it was conducted on mice, not humans. I do not usually refer to animal studies in my posts, for two reasons: Firstly, I consider animal research to be profoundly unethical. The most recent comprehensive assessment of the number of animals used for scientific purposes worldwide was published in 2020 but was based on statistics from 2015. It estimated that in that one year alone, over 192 million animals (excluding invertebrates) were bred and kept in captivity, genetically modified, intentionally maimed, poisoned, deliberately over- or underfed and subjected to unhealthy and species-inappropriate diets, irradiated, electrocuted, tortured in various and sundry other ways, and ultimately, in most cases, slaughtered (the euphemism used in the industry is ‘sacrificed’), mostly so that humans could learn more about stuff they probably shouldn’t be taking, eating or doing in the first place.
The second reason that I generally don’t refer to animal experiments is that mice, rats and dogs ain’t human. One of the most persuasive criticisms made by anti-vivisectionists against medical experimentation on animals, is that it is next to useless at identifying drugs that actually work in humans. Less than one in one thousand new drug candidates ever end up as approved medicines, and one of the chief reasons for this high failure rate is that tests conducted on animals are incredibly poorly predictive of safety and efficacy in human beings. In fact, a mere six per cent of animal studies are translatable to human response. And worryingly,
“Despite efforts to improve the predictability of animal testing, the failure rate has actually increased.”
Lost in translation: the valley of death across preclinical and clinical divide – identification of problems and overcoming obstacles
All that said, there are sufficient biological similarities between rodents and humans, for findings from animal feeding studies to have some relevance to human health. At the very least, they point to hazards that people who adopt the eating patterns used in such studies – and their healthcare providers – should be alert to.
And since we already have confirmation from studies conducted in humans, that some of the adverse effects of long-term consumption of a ketogenic diet by mice, documented in this study, do indeed occur in people (more on that later), those hazards are far from theoretical.
Why don’t researchers just conduct diet studies on humans? After all, few people care which dietary patterns result in optimal health for mice. It’s human outcomes that humans care about. But there are a few things that researchers can do to animals, that they can’t do to humans:
- They can completely control their diets; and they can do it long-term – even for the animal’s entire lifetime. The only experimental design for human studies in which researchers can exert total control over what participants eat is the metabolic ward study, in which volunteers live in a locked hospital ward for a period of time, during which they can only consume the meals provided to them. These studies are insanely expensive, and can only be continued for a few weeks at a stretch since participants must completely forego their normal lives for the duration of the study.
In the bad old days, researchers frequently made use of captive populations such as prisoners, patients of mental asylums and boarding school students to conduct long-term dietary experiments; nowadays, hell would freeze over before such a proposal passed ethics committee review. Ethics committees, however, have no problem with approving research projects that entail keeping mice on a particular diet for weeks, months or until they die (or are killed). And since a mouse lifespan is two years or less, it’s completely practical to study the lifelong, and even multigenerational, effects of a particular, precisely-defined dietary pattern on this species. And, - They can control for all other factors, so that the only variable is diet. In humans, diet-styles cluster with other lifestyle factors. For example, vegetarians are less likely to smoke and more likely to exercise regularly than meat-eaters, making it difficult for researchers to ascertain whether their health advantages – such as a lower risk of cardiovascular disease – are truly due to eschewing meat. But the living conditions of experimental animals can be tightly controlled, such that the only difference between one group and another is their diet.
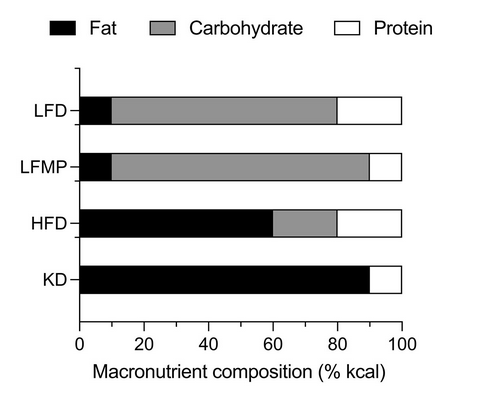
All that said, let’s dig into the recently-published paper, ‘A long-term ketogenic diet causes hyperlipidemia, liver dysfunction, and glucose intolerance from impaired insulin secretion in mice‘. The study documented the metabolic effects of four different feeding patterns – a standard low-fat diet, a low-fat moderate protein diet, a high-fat diet, and a ketogenic diet – as well as the effects of switching animals from one dietary pattern to another at various points in their lifespan. Adult male mice were fed ad libitum – that is, offered as much food as they wanted to eat – on the assigned intervention diet for 36 weeks – one-third of their potential lifespan – and female mice for 44 weeks. The distribution of macronutrients on each of the diets is shown below:
The study examined many facets of the animals’ metabolic function, as follows:
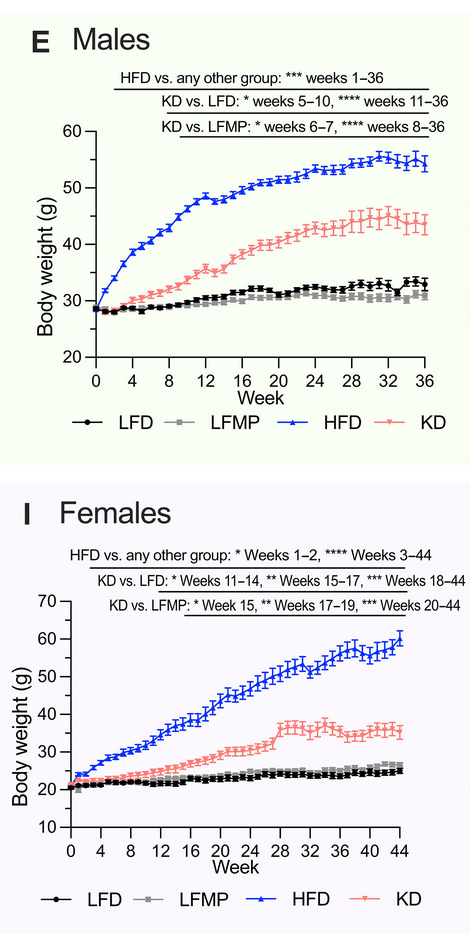
1. Weight gain
The ketogenic diet caused less weight gain than the high-fat diet, but more than either version of the low-fat diet. Weight gain took longer to get underway on the ketogenic diet, whereas the high-fat diet made mice gain weight almost immediately:
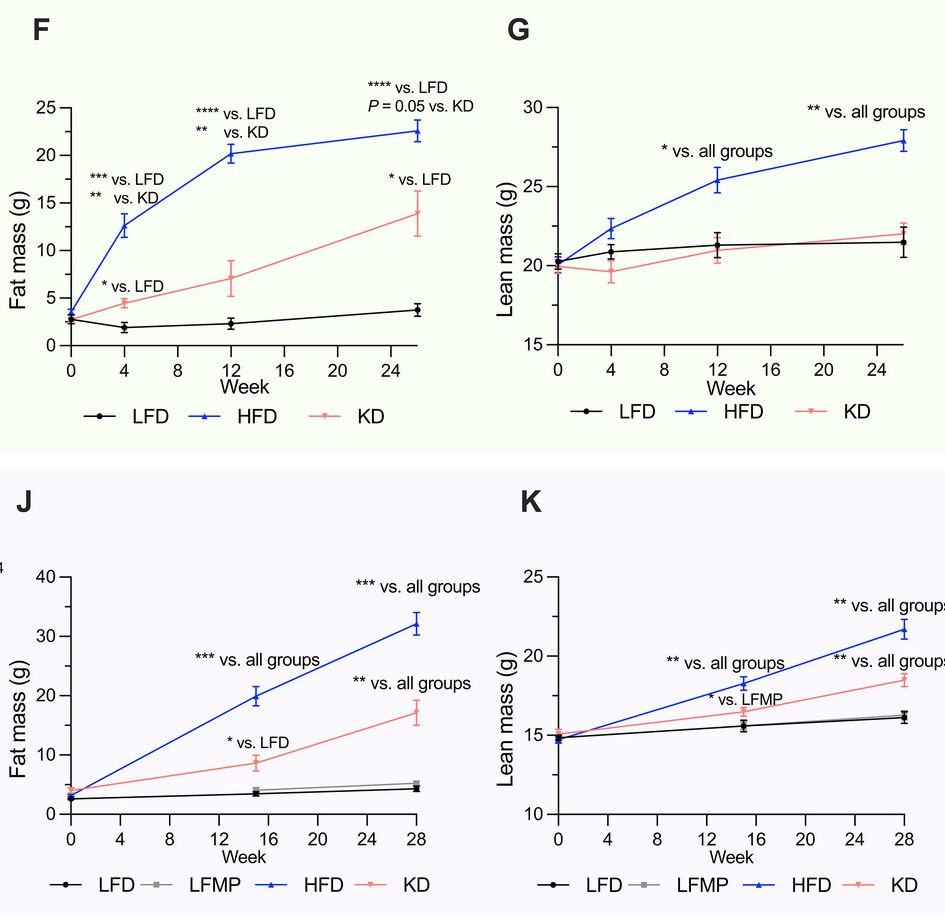
2. Body composition
Most of the weight gain in female mice on the ketogenic diet, and all the gain in males, was from fat mass. Mice on the high fat diet gained both lean and fat mass:
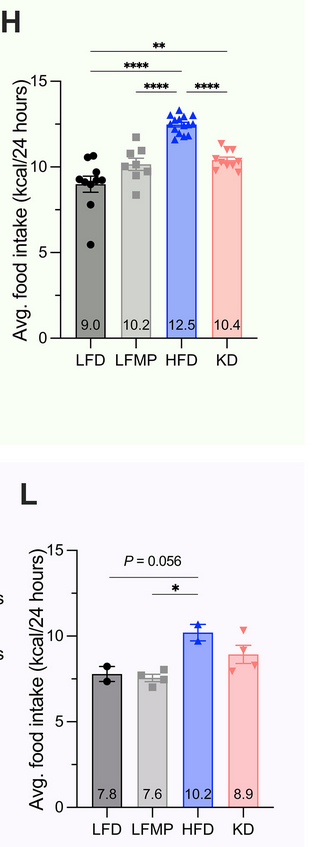
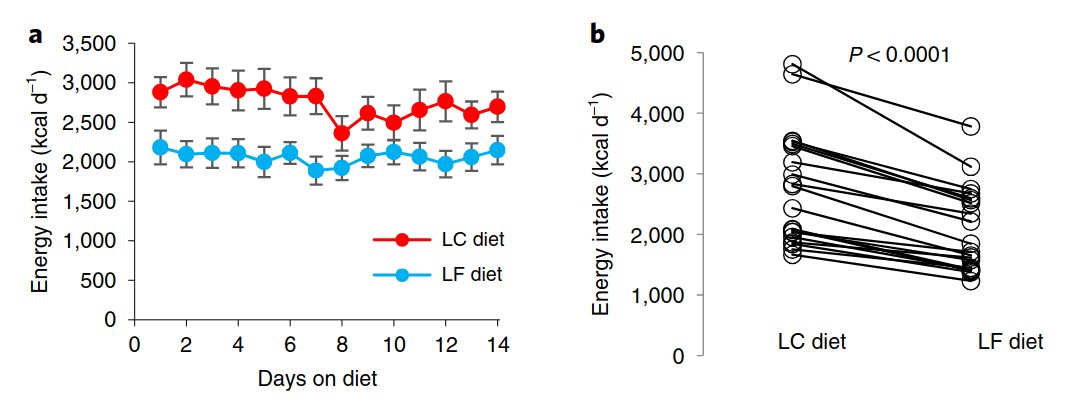
3. Energy intake
Contrary to the ‘metabolic advantage’ claims made by ketogenic diet enthusiasts (which I debunked in Ketogenic diets: Part 3 – Weight loss), the physics of weight gain is really quite simple: if you consistently take in more energy than you expend, you will gain weight. So it’s interesting to see how much food the mice ate on the four different dietary patterns. Remember, they were fed ad libitum meaning that they could eat as much as they wanted; as you can see, the mice assigned to either of the two low-fat diets ate the fewest calories, while those on the high-fat diet ate the most:
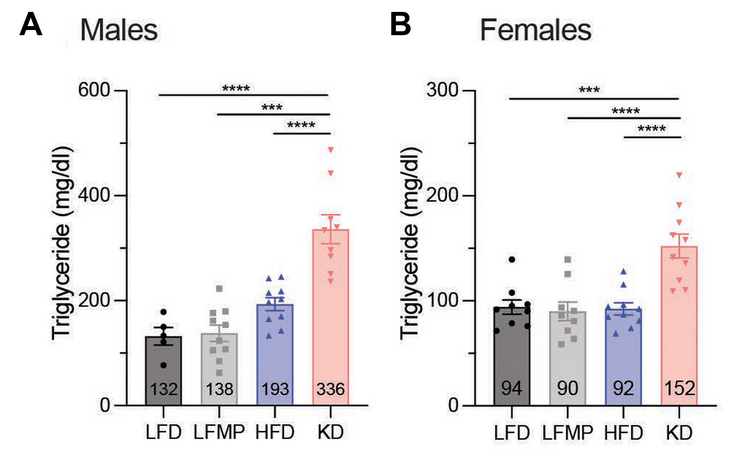
4. Triglyceride levels
The ketogenic diet caused dramatic elevations in triglyceride (blood fat) levels in both male and female mice. Interestingly, triglyceride levels were higher on the ketogenic diet than on the high-fat diet, even though body weight and body fat gains were greater on the high-fat diet. High triglycerides are one of the diagnostic markers of the metabolic syndrome.
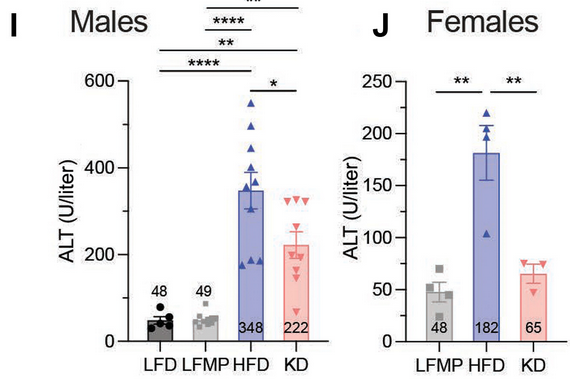
5. Liver function
Male mice developed hepatic steatosis (fatty liver) and elevated plasma alanine transaminase (ALT), an indicator of liver damage, on both the high fat and ketogenic diets, while liver inflammation was seen in both sexes:
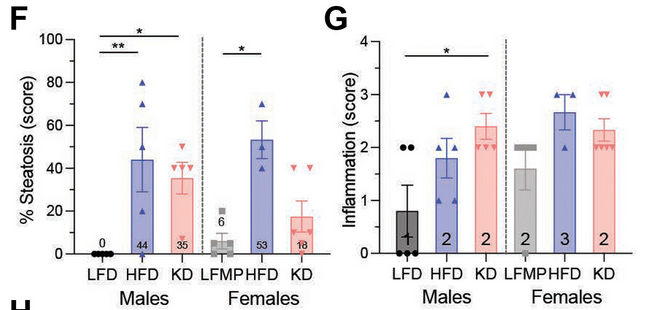
Analysis of the liver transcriptome (gene expression patterns) found that genes associated with steatosis, fibrosis, and inflammation were similarly upregulated in mice on both the ketogenic and high-fat diets, compared to mice on low-fat diets. Of the top 200 genes that were differentially expressed between mice on the ketogenic diet and mice on the low-fat diet, the gene expression patterns were virtually identical for the high-fat and ketogenic diets.
6. Glucose intolerance and insulin secretion
Mice fed the ketogenic diet initially had lower fasting blood glucose levels than mice on the high-fat diet, and lower postprandial (after-meal) blood glucose levels than mice fed a low-fat diet. But over time, the keto mice’s fasting blood glucose became elevated. Furthermore, mice on both the high-fat and ketogenic diets also became progressively more glucose intolerant (meaning they were not able to return to normal blood glucose levels after a dose of carbohydrate):
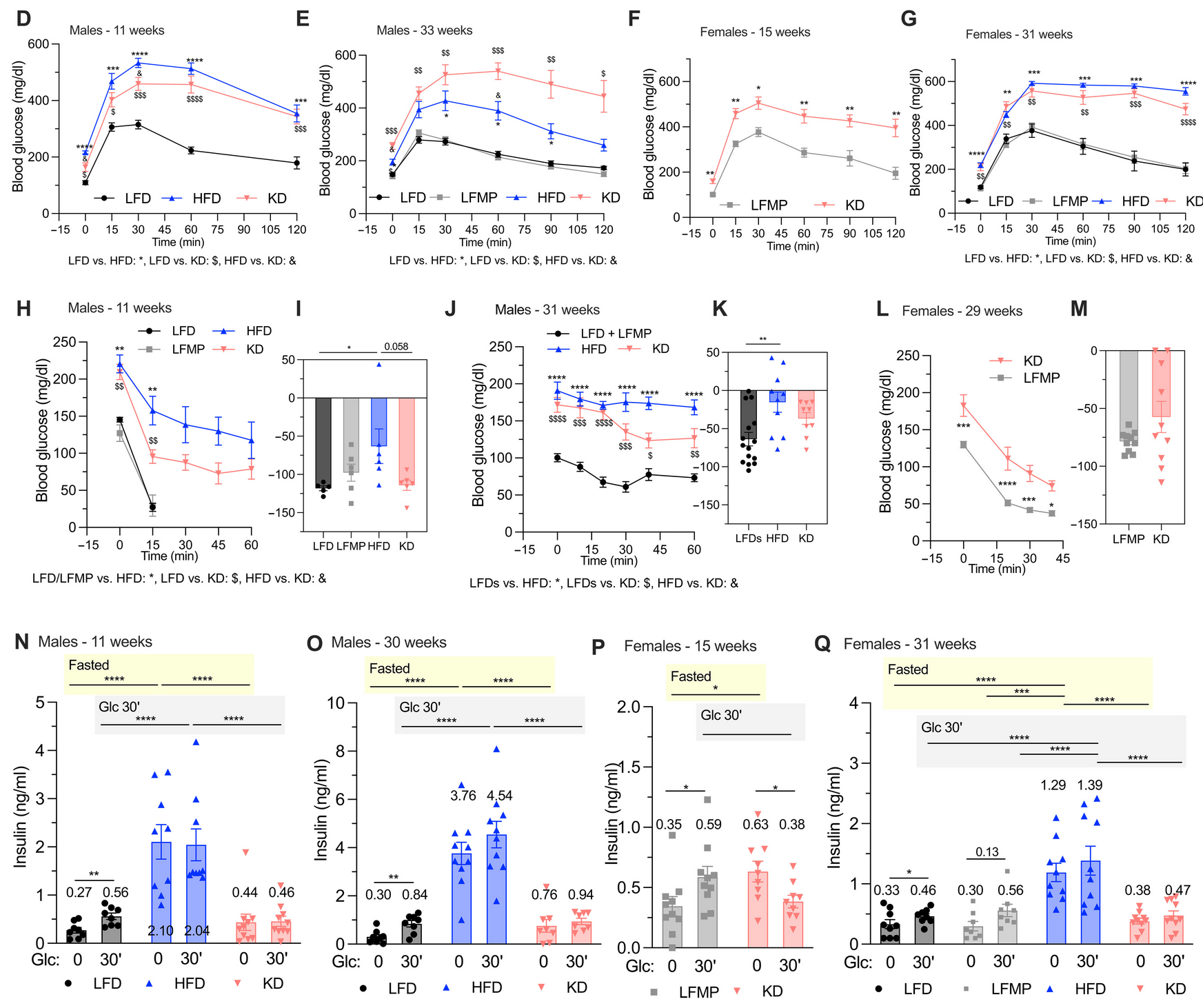
However, there was a crucial difference in the cause of this glucose intolerance. Whereas mice on the high-fat diet became more and more insulin resistant, mice fed a ketogenic diet retained their insulin sensitivity. But their ability to secrete insulin became progressively more impaired, even though they had the same number of insulin-secreting cells in their pancreas as mice on low-fat diets, and the same content of insulin within these cells.
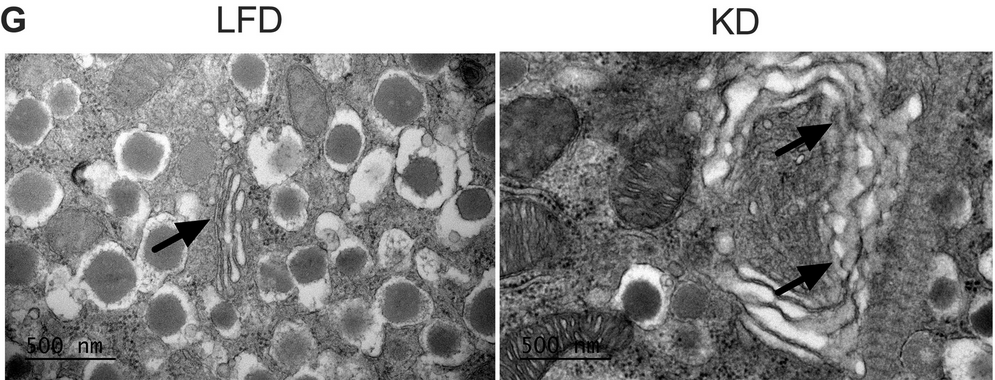
Analysis of the transcriptome revealed that mice fed a ketogenic diet had significant upregulation of genes involved with the Golgi apparatus and endoplasmic reticulum, two organelles within cells that produce, modify, package and transport proteins. Electron microscopy images of sections of pancreas from the mice, found that the Golgi apparatus in the insulin-secreting β cells of those on the ketogenic diet appeared dilated, swollen and fragmented compared to those on the low-fat diet. The researchers hypothesised that the ketogenic diet had disrupted endoplasmic reticulum-Golgi protein trafficking, causing defective transport and secretion of insulin granules.
The long and the short of it is that while the ketogenic diet limits weight gain, it severely impairs insulin secretion, progressively destroying the animals’ ability to regulate their blood glucose levels.
7. Restoring healthy body weight and metabolic function after obesity
In mice who had been made obese by 14-15 weeks of high-fat diet feeding (60 per cent fat), a low-fat diet caused more weight loss than a ketogenic diet. The low-fat diet also restored glucose tolerance and capacity to secrete insulin, whereas these remained impaired in mice switched from a high-fat to a ketogenic diet:
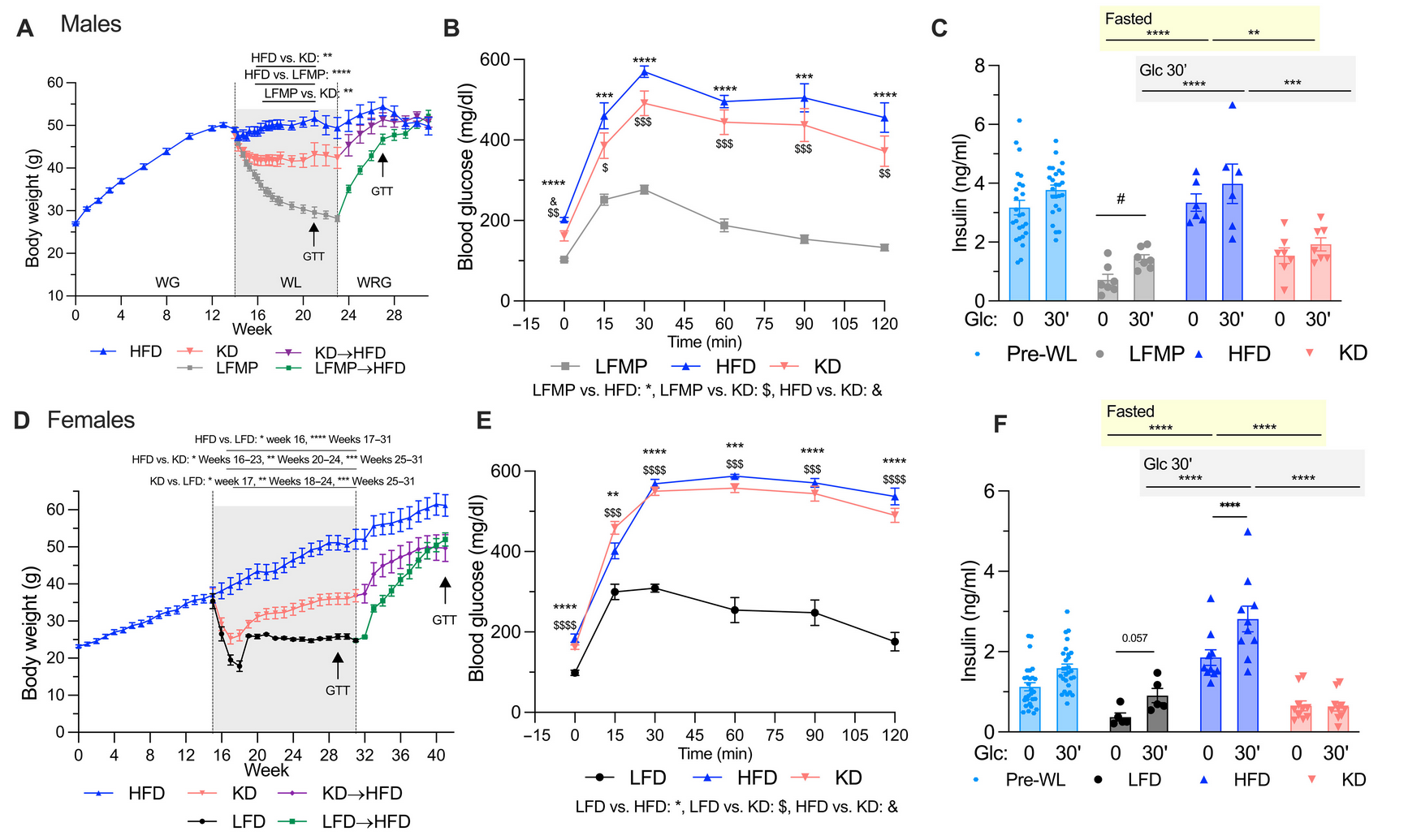
Mice that had been made obese on a high-fat diet, then lost weight on a ketogenic diet, remained hyperlipidemic while those switched to low-fat diets had lower triglyceride and cholesterol levels.
Pulling their findings together, the researchers concluded
“In summary, these findings show that while a KD [ketogenic diet] causes WL [weight loss] following diet induced obesity, it cannot cure or permanently ablate glucose intolerance or impaired insulin secretion. Although the effects of KD are reversible, these experiments show that a LFD [low-fat diet] more favorably affects glucose tolerance, insulin secretion, and WL.”
“Moreover, we observed worsening glucose intolerance and impaired insulin secretion the longer the animals had been on KD, so the vision of KD as a treatment for metabolic disease should be questioned even if initial improvements in health are observed. Although we found that glucose intolerance caused by a KD is reversible, it is possible that other effects may persist. Moreover, in mice with diet-induced obesity, a traditional high-carbohydrate LFD caused greater WL than a KD while improving glucose intolerance… While a KD can prevent and treat obesity, it causes hyperlipidemia, hepatic steatosis, and glucose intolerance. Unlike mice on HFD [high-fat diet], the mice on KD do not have detectable insulin resistance or hyperinsulinemia. Instead, they have impairments in insulin secretion due to a blockade in protein trafficking resulting from dilation of the Golgi apparatus, which also causes ER/Golgi stress.”
A long-term ketogenic diet causes hyperlipidemia, liver dysfunction, and glucose intolerance from impaired insulin secretion in mice
But what about humans?
If you keep pet mice, you now know that in order to keep them healthy, you definitely should not be feeding them a ketogenic or high-fat diet. But what evidence do we have that the metabolic harms inflicted on mice by the ketogenic diet, also occur in humans? Quite a bit, as it turns out.
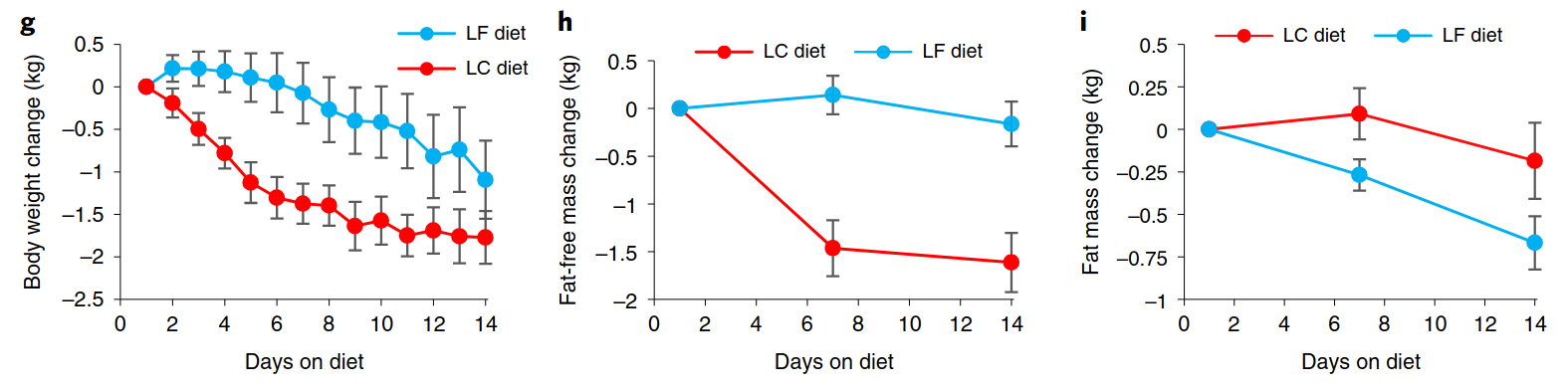
A ketogenic diet is less effective for weight loss and body fat reduction in humans than diets higher in carbohydrate, and lower in fat
As I discussed in Ketogenic diets: Part 3 – Weight loss, a metabolic ward study published in 2016 found that a relatively high-carbohydrate baseline diet (50 per cent carbohydrate, 15 per cent protein, 35 per cent fat) caused more body fat loss than a ketogenic diet, in overweight and obese men and fat-free mass (muscle, bone and vital organs) declined on the ketogenic diet.
And a truly low fat diet (10 per cent fat, 75 per cent carbohydrate, 15 per cent protein) caused more body fat loss than a ketogenic diet, while preserving lean mass, which declined on the ketogenic diet. Participants, who were instructed to eat ad libitum, spontaneously ate on average 689 fewer calories per day while on the low-fat diet than on the ketogenic diet, mirroring the results of the mouse study.
Humans on a ketogenic diet have impaired glucose tolerance and elevated triglycerides
In the low-fat vs ketogenic diet study referred to in the previous section, impaired glucose tolerance was noted after just two weeks on a ketogenic diet. A longer-running study conducted in free-living adults found the same thing: impaired glucose tolerance after four weeks, and twelve weeks, on a ketogenic diet.
In addition, triglyceride levels were elevated at these time-points. Elevated triglycerides were also found in young, normal-weight women after four weeks on a ketogenic diet. And this shouldn’t have come as a surprise to anyone: The original medical application of ketogenic diets was for the management of intractable epileptic seizures, and it has been known to increase triglyceride levels in children who were prescribed the diet for this reason, for decades.
A ketogenic diet can cause fatty liver and elevated liver enzymes
In a retrospective case review of 141 children placed on a long-term ketogenic diet for treatment of intractable seizures, 5.7 per cent suffered some type of liver-related side-effect; among these were elevated liver enzymes and hepatic steatosis (fatty liver).
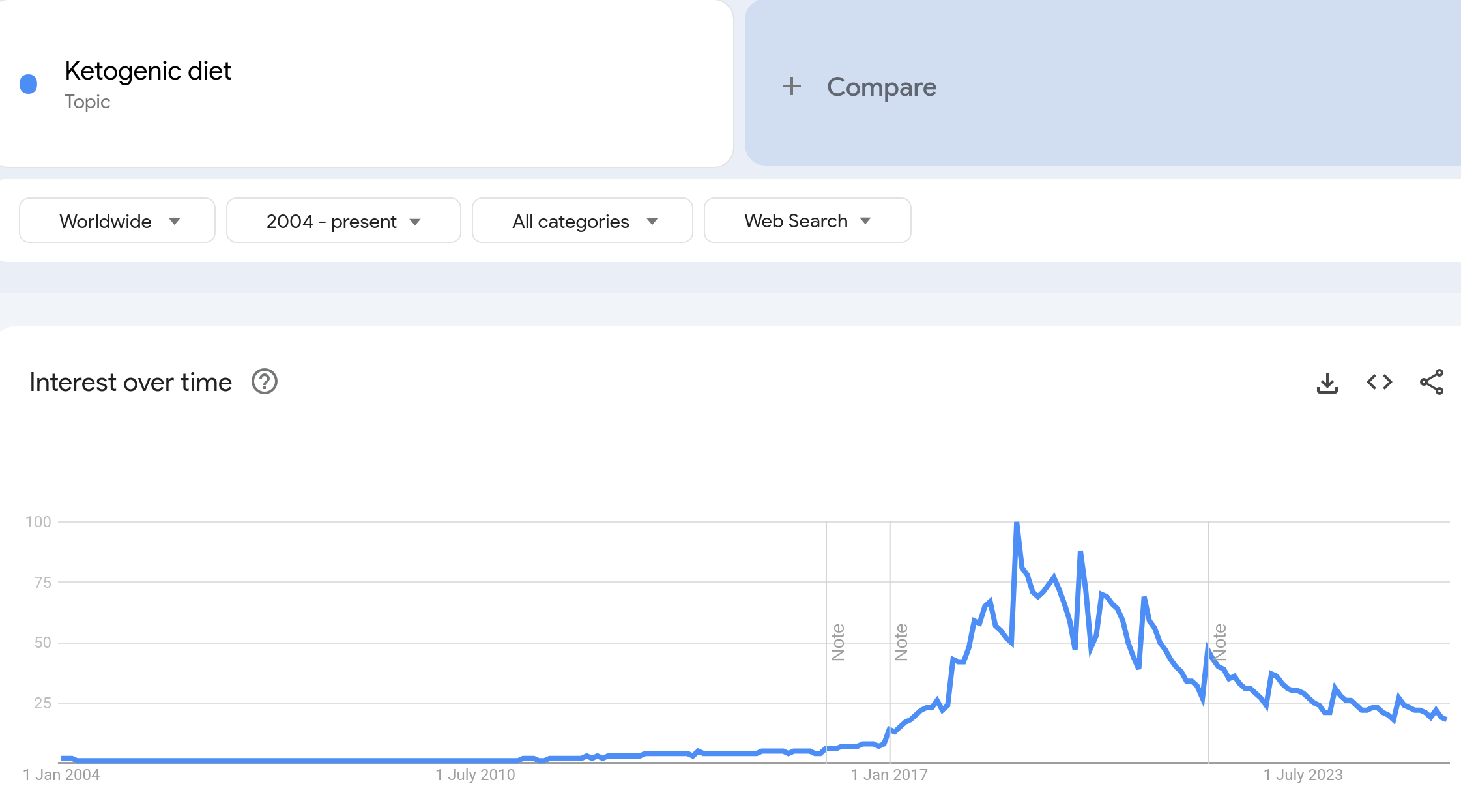
Why should we care?
OK, so there appear to be some pretty gnarly consequences of the ketogenic diet, especially when followed long-term. But does it really matter? Public interest in the ketogenic diet appears to have waned, if Google search trends are anything to go by:
But a highly vocal contingent of doctors, bloggers and ‘health influencers’ continues to aggressively promote the ketogenic diet, and they have an especially strong presence within the so-called health freedom community. I subscribe to the Substacks of many of the health professionals, journalists and other public figures who became dissidents during the COVID insanity, and have been dismayed to find that a considerable proportion of them endorse ketogenic diets for weight loss and treatment of cardiometabolic diseases such as diabetes.
It’s quite gobsmacking that so many people who were outraged about the lack of informed consent offered to people who received experimental modified RNA injections marketed as ‘vaccines’, don’t seem to hold the same perspective on diet advice. If you are going to recommend a ketogenic diet to anyone, you are obligated to offer informed consent – that is, to discuss the risks and benefits of treatment. Examining the totality of the evidence base for ketogenic diets, my conclusion is that the benefits are small and temporary, and the risks are unacceptably high. As I discussed at length in my ketogenic diet series, this way of eating is not ‘natural’, is inferior to higher-carbohydrate dietary patterns for weight loss and treatment of diabetes and cancer, and has harmful effects on the gut microbiota.
If your doctor, personal trainer or nutrition adviser recommends a ketogenic diet, my advice is to sack them and find someone better-informed.



