New research explores the link between oral contraceptives, emotional eating and binge eating
I’ve written extensively about the harmful effects of the oral contraceptive pill on women’s physical health and psychological well-being:
- Hormonal contraception and women’s mental health
- More evidence that taking the Pill in your teens is linked to depression
- This is your brain on the Pill
- More proof that the oral contraceptive pill causes depression
- New study finds all forms of hormonal contraception raise breast cancer risk
- How the Pill and HRT affect your gut… and your risk of autoimmune and inflammatory disease
And now, new research published in JAMA Network Open has added another risk to Pill users, on top of depression, anxiety, breast cancer, autoimmune disease, a shrunken hypothalamus and blunted stress reactivity: binge eating.
Binge eating is defined as “consumption of a large amount of food, in a short period of time, with a loss of control over eating”.
Many women report some changes in appetite and in the intensity and target of food cravings, associated with the phases of their menstrual cycle. Unfortunately for those who would like to justify devouring a family-sized block of Cadbury’s Dairy Milk in one sitting by attributing it to a biological requirement for chocolate (trust me, more than a handful of clients have tried this one out on me), it turns out that premenstrual chocolate cravings are in fact a purely cultural phenomenon. Only four per cent of Spanish women vs forty per cent of American women report premenstrual chocolate cravings, with immigrants to the US reporting more intense chocolate cravings, the more they become acculturated.
However, there does appear to be a biological basis for overeating, binge eating and emotional eating1 in the second half of the menstrual cycle, between ovulation and the onset of menstruation. The steroid hormones produced by women’s ovaries regulate reward systems in the brain, that use dopamine and opioids to reinforce consumption of high-calorie foods – especially those rich in fat and/or sugar. These reward pathways always fire off when we eat highly-palatable foods like chocolate, ice cream, cheese, processed meats and pastries, but they show increased activation in the post-ovulatory phase of women’s menstrual cycles.
The combination of higher estradiol2 and low progesterone levels in the preovulatory phase of the menstrual cycle tends to reduce food intake, while the post-ovulatory hormonal milieu of high estradiol and high progesterone is associated with increased food intake in both humans and non-human animals – especially of hyperpalatable food. And episodes of both binge eating and emotional eating occur more often in the postovulatory than the preovulatory phase.
OK, so women’s own ovarian-derived hormones can influence their propensity to overeat and binge eat. But what about the synthetic versions of estradiol and progesterone that more than 100 million women around the world take every day, in the form of oral contraceptives? That is, does being on the Pill cause women to binge eat or overeat for emotional reasons, more often than they otherwise would?
To find out, researchers recruited 422 women from the Michigan State University Twin Registry, who were already taking combined oral contraceptives (i.e. formulations that contained both a synthetic estrogen (most commonly, ethinyl estradiol) and progesterone (progestin). Only women using monophasic oral contraceptives (that is, those that provide a constant dose of synthetic estrogen and progestin across active pills) that contain 21 active pills and seven inactive or placebo pills per packet, were included, in order to narrow down the specific impact of a high-estrogen, high-progesterone hormonal milieu vs a low-estrogen, low-progesterone milieu, on the propensity to binge eat. Monophasics are also the most commonly-prescribed oral contraceptives, making the findings of this research very broadly applicable to Pill users.
For 49 consecutive days – incorporating two active-to-inactive pill transitions – participants filled in nightly online questionnaires on their eating behaviour, degree of weight preoccupation (mental fixation on dieting, weight, or body shape) and experience of negative affect (low mood and distressing emotions such as sadness, disgust, lethargy, fear, and distress) during the preceding day.
There was a marked increase in the frequency of emotional eating on the 21 days when participants were taking the active hormone pills, compared to when they were in the seven-day inactive pill phase. 51 of the participants were identified as experiencing clinically defined binge-eating disorder as per Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V), and these participants also had substantially more frequent episodes of emotional eating whilst taking active hormone pills. This association between emotional eating and active hormone pill-taking was not accounted for by changes in negative affect or weight preoccupation, indicating that it was driven by the specific hormonal milieu of high (synthetic) estrogen and progesterone.
Interestingly, emotional eating episodes were less frequent during the second oral contraceptive pill cycle than the first:
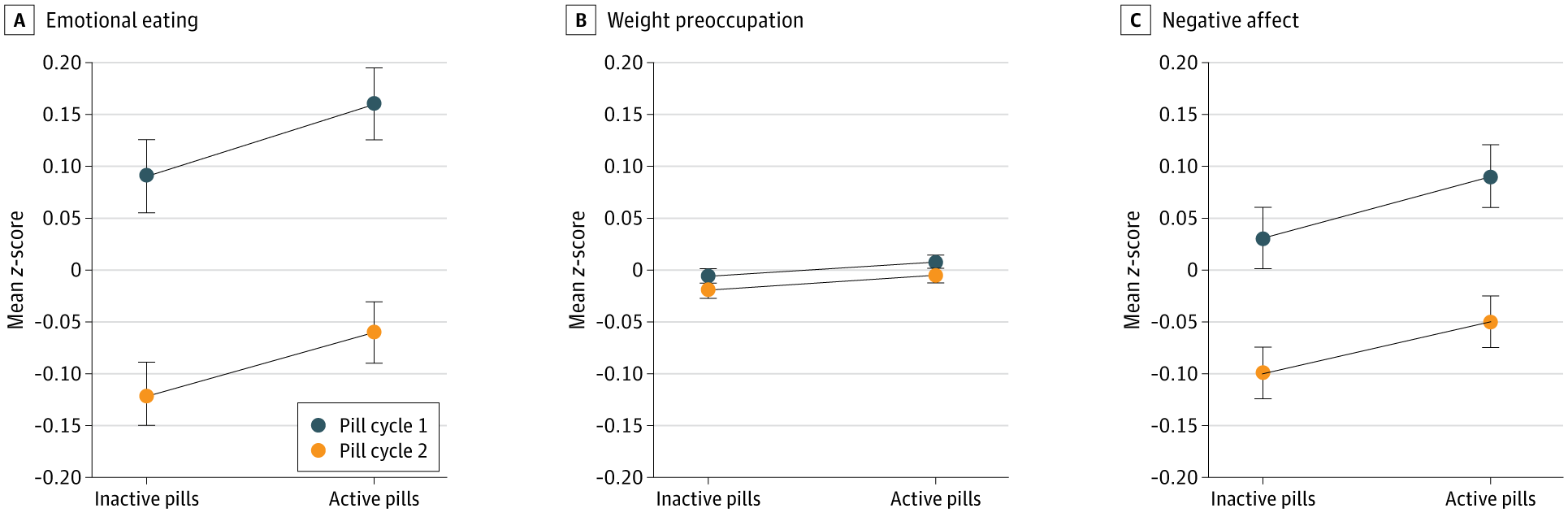
The researchers speculated that self-monitoring – the act of paying attention to one’s eating behaviour, and being accountable for it through daily reporting – may have decreased the frequency of emotional eating episodes in the second Pill cycle, as this has been reported in previous research.
Notably, not all women experienced increased frequency of emotional eating while on active hormone pills. Individual differences in genetic factors such as hormone metabolism or receptor activity, in epigenetic factors such as prenatal stress imprinting, or in early life experiences – or some combination of these factors – may conspire to make some women more susceptible to Pill-induced emotional eating and binge eating.
So if you’re struggling with binge eating, emotional eating or overeating, or a woman you love is battling with these disordered eating behaviours, the oral contraceptive pill might be part of the problem. This issue should be raised with the prescribing doctor, and you may want to print out the JAMA Network Open article and take it to the appointment.
Are you confused by the scientific claims and counter-claims that you encounter through popular and social media?
Would you like to learn how to read scientific research, assess its
biases, and understand how it fits within the body of scientific
literature? My EmpowerEd membership program is custom-made for you. Activate your free 1-month trial today!
- Emotional eating is defined as “the tendency to overeat or binge eat in response to negative emotions.” ↩︎
- Estradiol is the most potent form of estrogen, and the most prevalent in premenopausal women. ↩︎



