Listen to the Influential Wellnesspreneur podcast interview with me on ketogenic diets:
Updated 7 November 2022
So far in this series, I’ve discussed the origins of the ketogenic diet and the biological role of ketone bodies (Part 1), whether living in a state of ketosis is normal and natural (Part 2), and whether ketogenic diets are effective for weight loss (Part 3). In this post, I’m going to dissect one of the major health claims made for ketogenic diets: that they reverse insulin resistance and effectively treat diabetes.
Ketogenic diets and diabetes
Claims that ketogenic diets effectively treat diabetes are rife on the Internet and in popular books. Keto enthusiasts claim that carbohydrate consumption is the cause of the insulin resistance that drives type 2 diabetes, and that also develops in type 1 diabetes.
Insulin resistance is known to be an important risk factor for the development of the complications of diabetes, both microvascular – diabetic eye (retinopathy), nerve (neuropathy) and kidney disease (nephropathy) – and macrovascular – coronary artery disease, peripheral arterial disease, and stroke.
Therefore, argue ketogenic diet advocates, removing carbohydrates from the diet effectively treats the cause of diabetes and its complications. Here is a typical example of this formulation of diabetes:
“Insulin resistance functionally manifests itself as ‘carbohydrate intolerance’. When dietary carbohydrate is restricted to a level below which it is not significantly converted to fat (a threshold that varies from person to person), signs and symptoms of insulin resistance improve or often disappear completely”.
Beyond weight loss: a review of the therapeutic uses of very-low-carbohydrate (ketogenic) diets
There are certainly studies which demonstrate the effectiveness of ketogenic diets for reducing various markers of diabetic control.
For example, one study compared a ketogenic diet with “unlimited amounts of animal foods (i.e., meat, chicken, turkey, other fowl, fish, shellfish) and eggs; limited amounts of hard cheese (e.g., cheddar or swiss, 4 ounces per day), fresh cheese (e.g., cottage or ricotta, 2 ounces per day), salad vegetables (2 cupfuls per day), and non-starchy vegetables (1 cupful per day)” to a low-glycaemic, reduced-calorie diet.
Those assigned to the ketogenic diet lost more weight than those assigned to the low-glycaemic, reduced-calorie diet. In addition, the ketogenic diet caused a greater drop in haemoglobin A1C (HbA1c – a marker of long-term glucose control) and a greater rise in high-density lipoprotein cholesterol (HDL-C, a marker of lower cardiovascular risk), and more participants assigned to the ketogenic diet were able to reduce or discontinue diabetes medication.
On the other hand, there was no significant difference between the groups in either fasting glucose or fasting insulin levels. This contradicts the carbohydrate-insulin hypothesis of diabetes, which proposes that eating a high-carbohydrate diet drives up blood glucose and insulin levels, while a very-low-carbohydrate, or ketogenic diet lowers both.
And, as mentioned in Part 3, an umbrella review of published meta-analyses and systematic review of trials of diets for weight loss in diabetics, published in 2022, found that “low-carbohydrate diets were no better for weight loss than higher-carbohydrate/low-fat diets.”
In fact, there are multiple lines of evidence contradicting the dogma that “carbs cause diabetes, so low-carb cures diabetes”.
Do ketogenic diets really “cure” diabetes?
Firstly, most intervention studies on ketogenic diets are short-term, but the limited evidence available from studies with longer follow-up periods indicates that the beneficial effects of ketogenic diets on biomarkers dissipate over time.
For example, in a study that randomised obese people to follow either a low-carbohydrate, high-protein, high-fat diet or a low-calorie, high-carbohydrate, low-fat (conventional) diet,
“Both groups had significant increases in insulin sensitivity at six months, but the values were not significantly different from base line at one year.”
A Randomized Trial of a Low-Carbohydrate Diet for Obesity
In other words, the initial improvement in insulin sensitivity on either type of diet was not sustained. A temporary improvement in diabetes biomarkers is not a “cure.”
The “gold standard” in medical studies is considered to be a randomised controlled trial (RCT). No RCTs of ketogenic diets for the remission of type 2 diabetes have ever been conducted. Proponents of the ketogenic diet often point to a non-randomised controlled study conducted by Virta Health as proof that the diet can indeed “cure” diabetes. This study claimed a 25 per cent remission rate for participants assigned to a ketogenic diet, defining remission as HbA1c below 6.5 per cent while taking no diabetes medications.
However, the 2022 umbrella review of published meta-analyses and systematic review of trials of diets for weight loss and remission of diabetes cited above, rated this trial as “very low certainty of evidence” and at “serious risk of bias”, noting the lack of randomisation, uncontrolled confounding, selection bias, incomplete outcome data in 22 per cent of participants, possible selective reporting, imprecision, imbalance between groups, and a dropout rate of 17 per cent.
It’s fair to say that at this point, there is no high-quality evidence that ketogenic diets are effective at putting type 2 diabetes into sustained remission.
But let’s look at the other side of the coin.
Does high carbohydrate intake cause diabetes?
Epidemiological, or population-based studies, consistently demonstrate that reducing carbohydrate intake, and replacing it with increased consumption of protein and fat, is associated with increased risk of diabetes:
- The rate of type 2 diabetes in China rose from 2.6 per cent in 2000 to 9.7 per cent in 2010, with the most dramatic rise occurring in urban areas. But rice and other grain intake has dropped dramatically in China over that time, while oil and animal product intake rose – as did obesity rates.
- Likewise, indigenous Mexican communities such as the Tepehuano, Huichol and Mexicanero were found to have zero diabetes just before the turn of the 20th century, while eating an extremely high carbohydrate diet consisting mostly of corn, beans, rice and squashes. Pima Indians living in Mexico on high-carbohydrate diets deriving on average 25 per cent of energy from fat and 11 per cent from protein, have less than one-fifth the prevalence of diabetes compared to Pima living in the US on a higher fat and protein, lower carbohydrate diet.
- The Health Professionals Follow-Up Study tracked over 40 000 US men who were free of type 2 diabetes at baseline for up to 20 years, and found that participants with the highest intake of animal protein and fat had more than double the risk of developing diabetes of those with the lowest intakes.
- Vegans – who almost by definition eat a high-carbohydrate diet – were found to have half the risk of developing type 2 diabetes as meat-eaters, even after adjusting for physical activity and body mass index – in other words, even fat, lazy vegans had a reduced risk of diabetes, due to eating carbohydrate-rich plant foods rather than carbohydrate-free flesh foods and eggs.
Do high-carbohydrate diets make diabetes worse?
In intervention studies, low-fat plant-based diets have been found to be superior to conventional diabetes diets which restrict carbohydrate intake.
- Diabetic men who were receiving insulin therapy were confined to a metabolic ward and were fed a restricted carbohydrate diet typically recommended to diabetics (20 per cent protein, 43 per cent carbohydrate, 37 per cent fat), followed by a very low fat, high carbohydrate diet (21 per cent protein, 70 per cent carbohydrate, 9 per cent fat) for the remainder of the study. Participants were instructed to eat more if they lost weight on the high carbohydrate diet, in order to factor out the effect of weight loss on insulin sensitivity. Every single patient reduced his daily dose of insulin while on the high carbohydrate diet, from an average of 26 units per day to 11 units per day, and several were able to discontinue insulin altogether. Despite the reduction in insulin, fasting and postprandial (after-meal) plasma glucose values were lower in most patients on the high carbohydrate diet than on the standard diabetes diet.
- In a 74-week clinical trial comparing a low-fat plant-based diet to a diet conforming to American Diabetes Association guidelines, the plant-based diet improved blood sugar and lipid levels more than the conventional (carbohydrate-restricted) diabetes diet recommendations.
- A systematic review of controlled clinical trials using plant-based diets for diabetes found that they significantly improved glycaemic control, despite (or perhaps because of) increasing carbohydrate intake by, on average, 14 per cent of total energy, while decreasing fat by 12 per cent.
What drives insulin resistance – carbohydrates or fat?
It’s been known since the 1930s that dietary fat decreases insulin sensitivity – or to put it another way, causes insulin resistance. Saturated fat, which is found mostly in animal products but also in coconut and palm oils, has the worst effect on insulin sensitivity. Epidemiological studies indicate that “subjects with higher intakes of fat are more prone to develop disturbances in glucose metabolism, type 2 diabetes or impaired glucose tolerance, than subjects with lower intakes of fat”, while experimental studies clearly demonstrated that diets high in fat impaired insulin sensitivity, while diets low in fat but high in carbohydrate improved it.
Insulin resistance is characterised by accumulation of lipids (fats) in muscles, the liver and eventually the pancreas:
- Muscles take up free fatty acids from the bloodstream to use as a fuel, and will take up more when fat is the primary macronutrient in the diet. However, when dietary fat intake is persistently high, the muscles begin to accumulate more fat than they can oxidise (burn as fuel), and this intramyocellular lipid accumulation results in the muscle cells becoming insulin resistant.
- Insulin resistance in the muscles increases fat deposition in the liver, causing the liver to become insulin resistant too. This hepatic insulin resistance drives the liver to continually release glucose, which triggers the pancreas to constantly secrete insulin, and it also results in raised levels of triglycerides (fats) in the bloodstream, worsening the fatty liver.
- The high circulating triglycerides also cause fat accumulation in and around the pancreas, killing off the insulin-secreting beta cells (“lipotoxicity”) and eventually resulting in inadequate insulin production. At this point, blood glucose levels rise and the symptoms of type 2 diabetes occur.
These 3 pathological manifestations of insulin resistance are all driven by “energy imbalance” – that is, consuming more energy than we use up in our daily activities. A wholefood plant-based diet – high in unrefined carbohydrates and low in fat – is, as mentioned in Part 3 of this series, the most effective dietary intervention for long-term weight loss ever published in a peer-reviewed journal. Even when instructed to eat ad libitum (that is, until they were full, with no portion control) and without being asked to increase their exercise level, overweight and obese participants in the BROAD Study were able to achieve average weight losses of around 12 kg in 1 year.
Which diet is best for the long-term health of diabetics?
Finally, it’s important to note that diabetics don’t die of diabetes per se; they die of its complications. The major cause of death in diabetics is cardiovascular disease, and a low-fat, plant-based diet is the only diet ever shown to reverse coronary artery disease.
On the other hand, ketogenic diets raise total and low-density lipoprotein cholesterol, and C-reactive protein (CRP).
A 2022 systematic review and meta-analysis of 14 prospective cohort studies, conducted in European, Asian and Middle Eastern populations and incorporating data from over 1 million participants, most of them followed up for over 10 years, found a linear relationship between total cholesterol level and the risk of dying of cardiovascular disease. That is, the higher your total cholesterol, the higher the risk of dying of a heart attack, sudden cardiac death, or other cardiovascular cause:
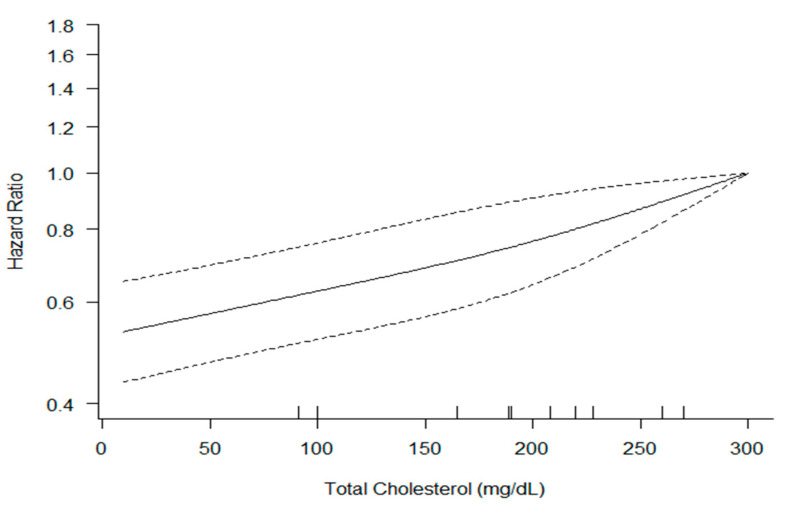
The same study found that those with the highest LDL-C have a 21 per cent higher risk of cardiovascular death than those with the lowest.
And among diabetics, elevated LDL-C is even more dangerous: for every 0.26 mmol/L (10 mg/dL) increase in LDL cholesterol, the risk of cardiovascular disease is increased by 12 per cent.
As for C-reactive protein (CRP), elevated levels are not only a predictor of developing diabetes in people who currently don’t have it, but a raised CRP in a person who already has diabetes is associated with an 84 per cent higher risk of developing cardiovascular disease, independent of how well their blood glucose is controlled.
In addition, children and young adults put on ketogenic diets to manage epilepsy were found to have stiffer arteries, an early marker of vascular damage, 1-2 years after commencing the diet.
These findings – elevations in total and LDL cholesterol, CRP and arterial stiffness – should sound the warning bell about the long-term cardiovascular risks of ketogenic diets, and rule them out as the gold standard for management of diabetes.
In summary, human populations living on high-carbohydrate, low-fat diets comprised primarily of minimally processed plant foods have historically enjoyed extremely low rates of diabetes. When societies make the “epidemiological transition” to a Western-style diet, which inevitably means a reduction in unrefined carbohydrates and an increased intake of animal foods and refined plant foods (including fats, oils, flour and sugar), their diabetes rates soar.
While ketogenic diets may lead to temporary improvements in glycaemic control, they lose their effectiveness over time, are fundamentally unnatural to humans (and all other animal species), and have no track record of preventing the life-threatening complications of diabetes.
Why take the risk of a ketogenic diet, when a wholefood plant-based diet is a delicious, sustainable and proven method of preventing, managing, and even reversing diabetes?
Confused about how to eat to prevent or reverse diabetes? Apply for a Roadmap to Optimal Health Consultation today!
Read Part 1, Part 2, Part 3, Part 5 and Part 6 of this series.



