20 June 2022
I’ve discussed early evidence that the experimental injections usually (but improperly) labelled “COVID-19 vaccines” may be having harmful effects on immune function and human-virus interaction in several previous articles, including What are COVID-19 injections doing to the human immune system?, Why COVID-19 “vaccines” will never end the pandemic, and Why Australia’s COVID-19 exit plan can’t succeed – Part 1 and Part 2.
In the last few months, the data on immune derangement by COVID-19 injections has built up from a few small stones to a giant avalanche of papers on pre-print servers and in peer-reviewed medical journals.
If you’ve read any of my previous articles (or, quite frankly, if you have more than two functioning brain cells left in your head and haven’t been asleep for the past 18 months) you won’t be surprised to learn that all the new data point in the same, worrying direction: the experimental injections are messing with the human immune system, and its complex interactions with SARS-CoV-2, in a number of dangerous ways.
There’s a lot of rather complicated science to discuss – so much so that it will take me multiple posts to cover it all – so I’ll start with an overview that zooms out from a micro to a macro view:
- COVID-19 injections not only generate a narrower immune response than natural infection, they also interfere with the development of the full suite of immune responses that would normally occur when a person contracts an infection and then recovers. Thus, people who experience “breakthrough infections” (which used to be labelled simply “vaccine failure” back in the good ol’ pre-Newspeak days) don’t develop the same broad and durable immune response as an uninjected person who gets infected with SARS-CoV-2 and recovers.
- This retardation of normal immune responses leaves injected people susceptible to getting reinfected, over and over again.
- Because the immune systems of injected people are fixated on attacking one part of the virus’ weaponry, mutated versions of the virus which evade those attacks are more likely to multiply within them, and find their way deep into vital organs, resulting in more severe illness.
- The mutated versions of the virus will also be expelled from the infected person’s body, and may find their way into the airways of other people. If those other people have also been injected, the virus will infect them more easily, multiply within them, and then be spread to other people. This “immune escape variant” of the virus will become the dominant version in populations with a high percentage of injected people.
OK, that’s the CliffsNotes version. Now let’s dig into the science.
Problem #1. COVID-19 injections induce narrow and short-lived immunity to SARS-CoV-2
1a COVID-19 injections inhibit the development of N antibodies
Back in November 2021, I mentioned a comment buried on page 23 of the UK Health Security Agency’s COVID-19 vaccine surveillance report for week 42:
“N antibody levels appear to be lower in individuals who acquire infection following 2 doses of vaccination.”
COVID-19 vaccine surveillance report: Week 42
To recap,
“The ‘N’ in ‘N antibody levels’ refers to the nucleocapsid protein, the ‘shell’ of the virus. ‘S antibodies’ form against the spike protein of the virus.”
What are COVID-19 injections doing to the human immune system?
Further explanation: The spike protein is used by the virus to gain entry to a host cell – like a Trojan horse being wheeled into a besieged city. Once inside the cell, the virus exposes its nucleocapsid protein, which is then used to hijack the cell’s protein-making apparatus in order to make more copies of the virus – as if the Trojan horse contained self-replicating soldiers who could overwhelm the city’s guards, and then burst out and attack neighbouring cities.
Going on,
“While people who have been jabbed but never infected will only develop S antibodies, people who have recovered from infection with SARS-CoV-2 will develop both N and S antibodies, giving them broad and durable protection to not just the currently-circulating strain/s of SARS-CoV-2, but future variants that develop as the virus does what viruses do – continuously mutates.
Or at least, COVID-recovered people should develop both N and S antibodies. But as the UKHSA report indicates, people who get infected after being ‘fully vaccinated’ (so-called breakthrough infections…) fail to develop the normal complement of N antibodies…
What does this mean? Quite simply, without N antibodies, ‘fully vaccinated’ individuals will be more susceptible to getting reinfected by strains of SARS-CoV-2 that have undergone mutation in the spike protein, which just happens to be the part of the virus that is mutating most rapidly due to vaccine-induced selection pressure.”
What are COVID-19 injections doing to the human immune system?
The UKHSA data that I referred to were observational, meaning that they weren’t gathered as part of an experiment with a set protocol and as such, are considered weak data that are merely hypothesis-generating.
For background, here’s a general map of how science proceeds:
- A scientist (which could mean any individual who employs the scientific method) makes an observation of a particular phenomenon, forms a hypothesis that might explain the phenomenon, then designs an experiment to test the hypothesis.
- If the results of the experiment appear to generally confirm the hypothesis, other scientists design experiments to refine and test it in larger and/or different populations and/or settings and/or under different circumstances. The more often these experiments yield results that favour the hypothesis, the greater its explanatory power is considered to be.
- Meanwhile, other scientists propose different explanations for the observed phenomenon, design experiments to test their competing hypotheses, and publish their results.
- After a period of years to decades, weaker hypotheses get knocked out, and the hypothesis with the greatest explanatory power comes to be generally accepted as ‘true’, at which point it is elevated to the status of a theory (such as Darwin’s theory of evolution by natural selection).
- In a comparatively small handful of very narrow cases, a theory may be further elevated to the status of a law (such as Newton’s Law of Universal Gravitation).
It turns out that, long before the observational UKHSA data were published, an experiment was being conducted which yielded data that powerfully confirm the hypothesis that COVID-19 injections interfere with the development of broad-spectrum immunity against SARS-CoV-2. That experiment was the Phase 3 trial for Moderna’s COVID-19 injection.
Just over 30 000 participants were enrolled in this trial; roughly half were assigned to receive two doses of the experimental mRNA injection and the other half received two doses of a saline placebo injection, 4 weeks apart.
To determine whether participants had become infected with SARS-CoV-2 during the trial, nasopharyngeal swabs for SARS-CoV-2 RT-PCR testing were collected at set intervals, as well as any time a participant reported a symptom of COVID-19. Blood samples to check for N antibodies were also collected from all participants at set intervals.
Researchers from the National Institutes of Health, Moderna and several major US teaching hospitals analysed these data on infections and immune responses, and published their findings on the medRxiv preprint server.
1789 participants were diagnosed with SARS-CoV-2 infection during the blinded phase (1298 placebo recipients and 491 vaccine recipients), as follows:
- 337 placebo recipients and 347 “vaccine” recipients were found to either have N antibodies to SARS-CoV-2 or a positive RT-PCR test at their first scheduled visit, when they received their first injection.
- 64 placebo recipients and 43 “vaccine” recipients were found to have N antibodies on Day 29 of the study, when their received their second injection, indicating that they had either become infected very shortly after their first injection, or had already been infected but had only seroconverted (begun producing N antibodies) following their first injection.
- 36 placebo recipients and 13 vaccine recipients tested positive on RT-PCR on Day 29 of the study.
- 754 placebo recipients and 58 “vaccine” recipients experienced illness 14 or more days after receiving both injections, and were diagnosed with SARS-CoV-2 infection using an RT-PCR swab obtained at a visit scheduled for the purpose of assessing their illness.
Those in the first and second groups were equally likely to have N antibodies by the end of the blinded study period (roughly 5 months after enrolment), indicating that – very fortunately – the Moderna shot didn’t impede the development of robust immunity in people in whom this process was well underway before they received both doses of the experimental product.
In the third group, 70 per cent of placebo recipients who tested positive for SARS-CoV-2 when they showed up for their second shot had developed N antibodies by the end of the blinded study period, compared to only half of participants who got the Moderna shot. The difference between the two groups failed to reach statistical significance, probably because of the small numbers of participants in this category.
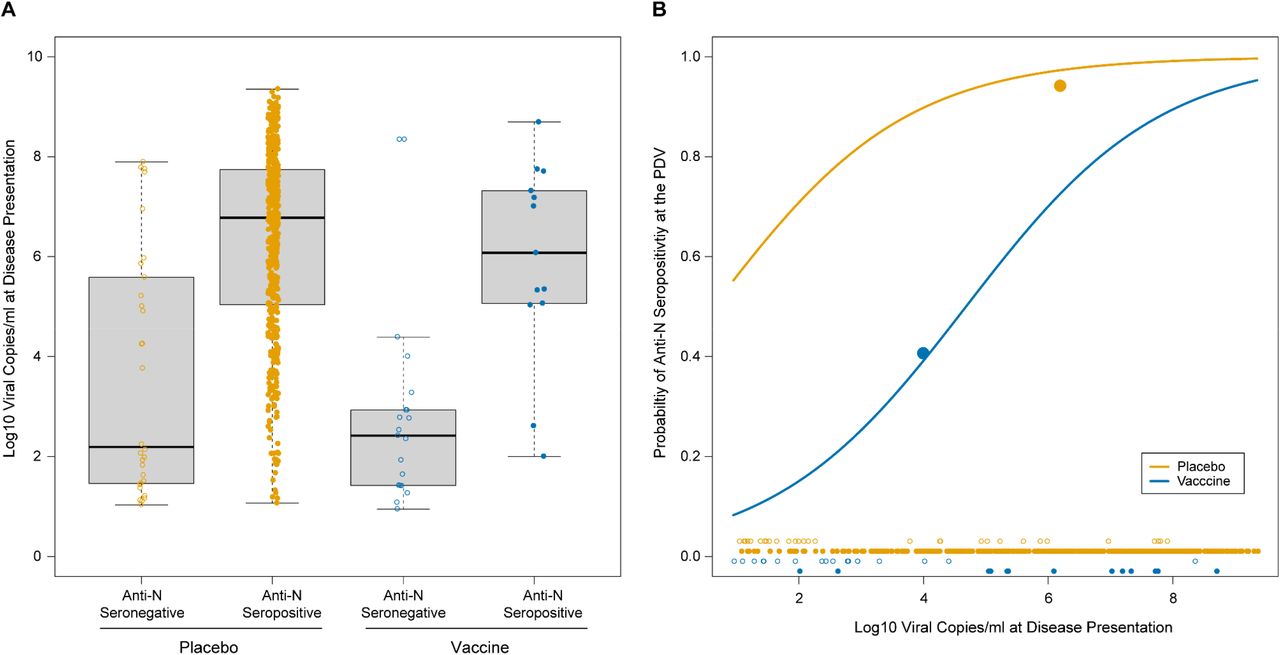
However, in the fourth group – people diagnosed with COVID-19 at an illness visit – by the end of the blinded study period, N antibodies were detected in the blood of only 40 per cent of those “fully vaccinated” with the experimental Moderna mRNA product (defined as two weeks post second shot), compared to 93 per cent of placebo recipients, and the difference was statistically significant. In other words, those who got infected after being “fully vaccinated” were less than half as likely to develop a broad immune response to SARS-CoV-2 than people who received the placebo.
Promoters of the experimental injections have attempted to fob off the growing body of evidence that injected people have a narrow immune response by arguing that when injected people get infected, they are able to fight off the virus much faster, resulting in shorter infections with a lower viral load, and therefore a dramatically lower exposure to N protein and in turn, less stimulation to produce N antibodies. In other words, they claim, the injections work so well that the recipient’s immune system doesn’t need to make N antibodies.
But that’s not what the Moderna trial data showed. The researchers used the cycle threshold (Ct) value of the RT-PCR test to estimate the number of viral copies that each person diagnosed with COVID-19 had. (I’ve explained the link between Ct and viral copies in detail here, but in brief, the lower the Ct, the more viral copies an infected person has.)
And no matter how many or how few viral copies participants had, those who received the placebo were dramatically more likely to develop N antibodies than those who got the Moderna shot:
“For any given viral copy number, the odds of anti-N seropositivity were 13.67 times higher for the placebo arm than the vaccine arm.”
Anti-nucleocapsid antibodies following SARS-CoV-2 infection in the blinded phase of the mRNA-1273 Covid-19 vaccine efficacy clinical trial
While 71 per cent of placebo recipients who had a mild infection (low viral copy number) developed N antibodies by the end of the trial, only 15 per cent of Moderna-injected people with the same viral copy number showed this evidence of robust and durable immunity to SARS-CoV-2.
And as Figure 2B (below) shows, while placebo recipients with very low viral copy numbers that would result in exceptionally mild – in fact, most likely asymptomatic – infections had an almost 60 per cent probability of developing N antibodies, it took almost 100 000 times as many viral copies for Moderna shot recipients to reach that same probability.
If you have that many viral copies, chances are you’re going to be feeling pretty ill (the more viral copies in your body, the more aggressively the immune system responds, generating fever, fatigue, aches and pains and all that other fun stuff that happens when you have a lurgy) and you’re also going to be shedding far greater amounts of virus onto other people.
Also, the severe reduction in N antibody production among Moderna jab recipients wasn’t a general marker of poor immune response to the injection; there was no significant difference in N antibody levels between people who produced high levels of antibodies to the spike protein (which is the aim of the injections) vs those who had low spike protein antibody titres.
To help you fully grasp why all of this matters, here’s a simplified explanation of how acquired immunity works:
In the process of fighting off viruses, certain cells in your immune system tear the virus’ genetic code into little pieces and show the snippets of code to other immune cells. These cells all memorise a different snippet and if they ever see it again, they recognise the virus that it belongs to and can easily fight the pathogen off using highly targeted strategies that they developed through their first encounter with it.
Just as a criminal could easily change his clothes, dye his hair or grow a moustache so he looks superficially different to his ‘WANTED’ poster photo, a virus can easily change certain pieces of its genetic code, evading detection by the immune cells that are looking for this specific piece of code.
But just as it’s much harder for the criminal to change the shape of his nose or remove the dimple in his chin – features that a detective is trained to pay close attention to – so there are pieces of the virus’ genetic code that are very resistant to change, and any immune cell that is looking for those pieces will quickly spot them if the virus has another crack at you.
And this rapid recognition results in a quick and comprehensive defence, so that you ended up having very mild or no symptoms of illness.
Conversely, if all the virus needs to do to fool your immune system is to swap its baseball cap for a Fedora, you’ll be prone to getting infected with it over and over again.
So, to summarise, the experimental Moderna injection retarded the development of a broad and robust immune response to SARS-CoV-2 in people who became infected despite being “fully vaccinated”, such that only those who became very sick and very contagious ended up with antibodies against both the spike and nucleocapsid proteins of SARS-CoV-2. On the other hand, the vast majority of placebo recipients who were exposed to SARS-CoV-2 during the trial developed both spike and nucleocapsid antibodies, even if they experienced mild symptoms or none at all.
Whilst multiple significant mutations in the spike protein of SARS-CoV-2 have developed since the virus made its debut in 2019, generating almost an entire Greek alphabet’s-worth of variants, the nucleocapsid protein is far more genetically stable. Hence, we could hypothesise that having both S and N antibodies is likely to be more protective against reinfection with SARS-CoV-2 variants than S antibodies alone.
1b COVID-19 injections do not elicit the formation of long-lived plasma cells
In the process of combating an infection by a virus that you’ve never encountered before (“primary immune response”), a type of immune system cell called a B cell, goes through a series of steps that ultimately result in the development of long-lasting immunological memory.
First, a “naïve” B cell which has the capability of recognising a snippet of the virus’ genetic code, is shown this snippet by another type of immune cell, called an antigen-presenting cell. This activates the B cell, which then begins to undergoes a series of modifications that result in it differentiating into plasma cells, memory B cells and long-lived plasma cells. Importantly, it’s the long-lived plasma cells that are responsible for rapidly ramping up antibody production in order to prevent infection if the virus is encountered again (“secondary immune response”).
However, according to two Italian researchers who conducted an exhaustive review of the published literature on the immune effects of COVID-19 injections,
“There is no evidence that these vaccines induce the production of long-lived plasma cells (LLPCs), in a SARS-CoV-2 virus naïve population.”
mRNA COVID-19 Vaccines and Long-Lived Plasma Cells: A Complicated Relationship
The researchers propose two explanations for the lack of long-lived plasma cells: immune cross-reactivity to other, endemic coronaviruses and antibodies to polyethylene glycol (PEG), an ingredient in both the Pfizer and Moderna injections. These hypotheses are beyond the scope of this article, but I encourage you to read their paper if you’d like to learn more.
The bottom line is this:
“Vaccination has a high chance of activating cross-reactive memory cells but little chance of eliciting LLPCs. The absence of LLPCs allows SARS-CoV-2 infection when the antibodies produced by plasma cells, derived from the activation of MBCs, vanish. Waning immunity seems to be already a concrete fact 4–6 months after completion of the vaccination cycle. Finally, with these vaccines, the elicited immune response is probably a secondary immune response, not a primary immune response with the natural production of LLPCs.”
mRNA COVID-19 Vaccines and Long-Lived Plasma Cells: A Complicated Relationship
The implication of the COVID-19 injections inducing a secondary rather than primary immune response is that those who receive them will never develop long-term immunological memory to SARS-CoV-2, with the capacity to respond to reexposure to the virus by rapidly escalating antibody production, which naturally falls to low levels within months after the initial infection has resolved.
Instead, they will become reliant on frequent re-“vaccination” to restore antibody levels to the point where they provide some protection against infection.
It’s immunity on subscription: the perfect business model for the injection manufacturers, but a lousy deal for the public because having constant high levels of circulating antibodies is profoundly abnormal and increases the risk of immune system dysregulations, such as autoimmune conditions (which have been reported with high frequency after COVID-19 injections).
So, is there solid evidence for the hypothesis that natural immunity outperforms injection-induced immunity, and that injected people are getting reinfected, multiple times? Yes, and we’ll dig into it in Part 2.
In the mean time, here’s some anecdata from the Twitterverse:




2 replies to "COVID-19 injections are screwing with immunity: Part 1"
What a gem of insanity that third tweet is!
It’s a doozy!