With Victorian premier Daniel Andrews unleashing a SARS-CoV-2 testing blitz on Melbourne suburbs labelled as COVID-19 ‘hotspots’, and Prime Minister Scott Morrison raising the threat of fines for those who refuse to be tested, it’s high time to put the vexed issue of testing under the microscope.
There are two broad categories of test for the novel coronavirus:
- Reverse transcriptase polymerase chain reaction (RT-PCR) tests aim to detect the presence of the virus itself, by identifying certain sequences of nucleic acids that make up its genetic code; and
- Serology tests, which detect indicators that the person’s immune system has mounted a defense against the virus by manufacturing antibodies, known as immunoglobulins M and G (IgM and IgG).
The Therapeutic Goods Administration (TGA), which is a branch of the Commonwealth Department of Health, has authorised a total of 67 test kits for SARS-CoV-2 detection, 25 of them being RT-qPCR.
The TGA acknowledges that there is limited evidence for the accuracy and usefulness of these tests:

The TGA also states that PCR tests should not be used to identify people who have been exposed to the virus but are not showing any symptoms (asymptomatic carriers):

RT-PCR tests
Importantly, it’s unclear whether a person who tests positive on the RT-PCR test is actually infected with it (i.e. is suffering from a clinical illness due to the virus):

This is important, since viruses are intracellular pathogens – that is, they can only make us sick if they manage to get inside our cells and hijack our cellular machinery in order to make more copies of themselves.
Detection of viruses in bodily fluids – which are, by definition, found outside cells – such as those collected in the nasal and/or oral swabs used for the SARS-CoV-2 RT-qPCR test does not equate to infection:
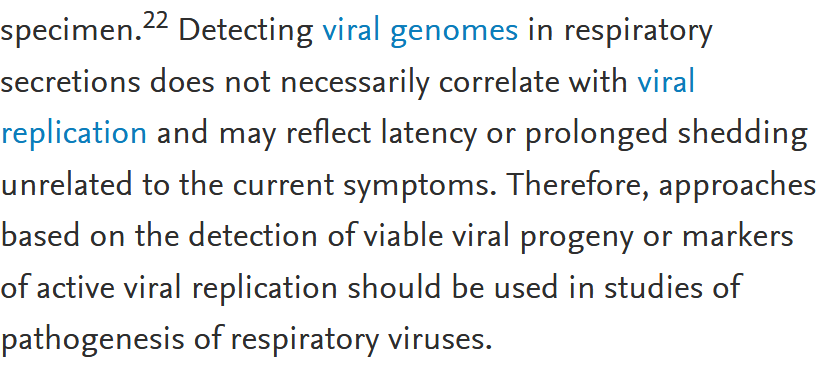
No such means for detecting viable viral progeny (that is, viral particles that are actually able to gain entry to cells and cause clinical illness) or markers of active viral replication yet exist for SARS-CoV-2.
The Instructions for Use accompanying a CDC-approved RT-PCR test for SARS-CoV-2 explicitly state that the test’s diagnostic value is dubious:

When even the Nobel Prize-winning scientist who invented the PCR test – Dr Kary Mullis – cautioned that the test should not be used to diagnose viral infections, one begins to wonder why the authorities would be threatening those who refuse to have one with A$10 000 fines.
Why did Mullis consider the PCR test unsuitable for diagnosing viral infection? Because it is essentially a manufacturing technique for DNA. It allows researchers to take a tiny amount of genetic material and rapidly make millions or even billions of copies of it, in order to study it in detail.
In the case of an RNA virus such as SARS-CoV-2, the RNA in the sample must first be converted into DNA, which is then put through repeated cycles of heating and cooling in order to amplify it.
However, the number of cycles that the sample will be put through in order to determine whether it is ‘positive’ or ‘negative’ for SARS-CoV-2 – the ‘cycle threshold’ – varies between different tests.
A higher cycle threshold means that there are very few copies of viral RNA in the sample (and therefore, presumably, less likelihood of both clinical illness and capacity to infect others), while a lower cycle threshold means that the sample contained more copies of viral RNA.
In an evaluation of one RT-PCR test currently being used in Australia, cycle thresholds of up to 40 were held to constitute a positive finding (i.e. presence of the virus) while cycle thresholds of 40-45 were considered to require further testing.
However, researchers from Harvard University have pointed out that
“Following complete resolution of symptoms, people can have prolonged positive SARS-CoV-2 RT-PCR test results, potentially for weeks… At these late time points, the Ct [cycle threshold] value is often very high, representing presence of very low copies of viral RNA… In these cases, where viral RNA copies in the sample may be fewer than 100, results are reported to the clinician simply as positive. This leaves the clinician with little choice but to interpret the results no differently than for a sample from someone who is floridly positive and where RNA copies routinely reach 100 million or more. A positive RT-qPCR result may not necessarily mean the person is still infectious or that they still have any meaningful disease. First, the RNA could be from nonviable or killed virus. Live virus is often isolable only during the first week of symptoms but not after day 8, even with positive RT-qPCR tests. Second, there may need to be a minimum amount of viable virus for onward transmission. For infection control purposes, the utility of the assay is greatest when identifying people who are floridly positive and at risk of further transmission.”
According to these researchers, patients with a cycle threshold of greater than 34
“likely do not have meaningful or transmissible disease.”
To Interpret the SARS-CoV-2Test, Consider the Cycle Threshold Value
However, as stated above, a test with a cycle threshold of up to 40 is approved for use in diagnosing COVID-19 in Australia.
A case report of four medical personnel treated for COVID-19 at Zhongnan Hospital of Wuhan University underlines the limitations of RT-PCR testing. All four had mild to moderate illness, and after a positive RT-PCR test for SARS-CoV-2, were quarantined at home. After their symptoms resolved and they had two negative RT-PCR tests, they were released from quarantine. All underwent subsequent RT-PCR testing, between 5 and 13 days after their quarantine period ended, and all 4 tested positive. Yet none had symptoms, and no one with whom they lived while in home quarantine became infected.
Serology tests
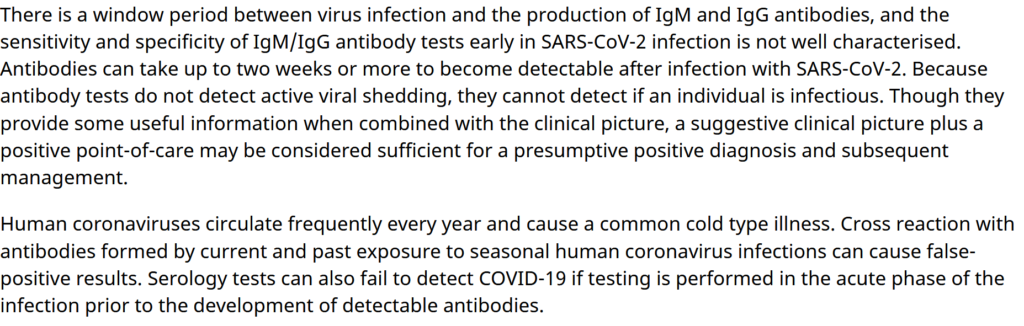
Serology (antibody) tests are next to useless for detecting current infection, cannot determine whether a person is contagious (able to pass the virus on to someone else; note that the TGA statement conflates ‘infectious’ with ‘contagious’), and may result in a false-positive diagnosis (i.e. wrongly indicate that a person has been infected with SARS-CoV-2) due to cross-reaction with genetic material from other widely-circulating types of coronaviruses that cause the common cold:
Sensitivity and specificity
The two primary metrics by which diagnostic tests are measured are sensitivity and specificity.
In terms that are meaningful to the present discussion, sensitivity is a measure of how many false negatives a test will generate – that is, how many people who do have SARS-COV-2 in their samples will be told that they don’t, while specificity is a measure of the test’s false positive rate – how many people will be told that they do have SARS-CoV-2 in their samples when in fact they don’t.
Positive and negative predictive values
While sensitivity and specificity are characteristics of tests, and hence do not vary (assuming that the test is carried out correctly), positive and negative predictive values are measures of the clinical relevance of a test.
Positive predictive value is the probability that following a positive test result, that individual will truly have that specific disease.
Negative predictive value is the probability that following a negative test result, that individual will truly not have that specific disease.
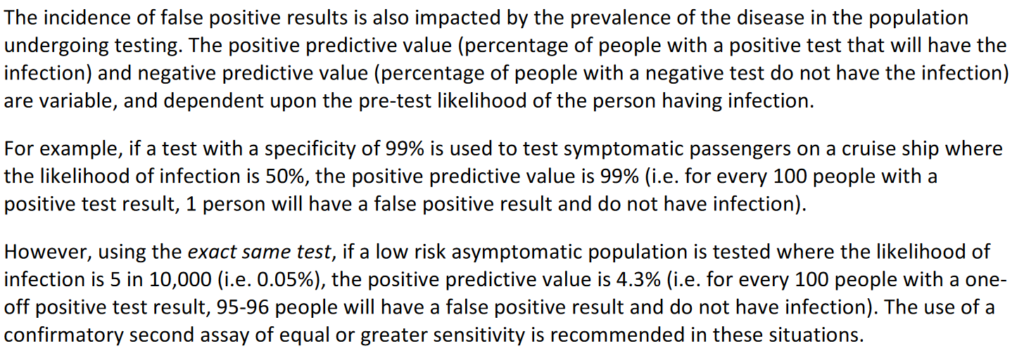
While the sensitivity and specificity of tests are fixed, the positive and negative predictive values of the test vary depending on the prevalence of the disease that’s being tested for in the population.
As the prevalence of the disease declines in a population, the positive predictive value decreases, meaning there are more false positives for every true positive. Conversely, as prevalence decreases, the NPV increases meaning there are more true negatives for every false negative.
A document issued by the Public Health Laboratory Network explains the problem:
Now do you see the problem with Premier Andrews’ aggressive testing policy? Going door to door to round up people who have no symptoms and coercing them to undergo testing, under the threat of a substantial fine, will inevitably result in hundreds, if not thousands, of people who do not have SARS-CoV-2 infection being told that they do.
Each of these people must then be notified to the authorities as a ‘case’, regardless of whether they have any symptoms whatsoever, leading to artificial inflation of the severity of the pandemic, which them becomes a justification for more draconian measures to control the spread of the virus.
It’s deeply disturbing that this self-evidently wrong-headed approach to testing is being actively promoted by Victoria’s Acting Chief Medical Officer.
The bottom line is that an RT-PCR test cannot determine whether an ill person’s symptoms are due to SARS-CoV-2 infection, and may falsely identify a well person as infected when he or she is not, with the risk of this false positive increasing as the prevalence of the virus decreases.
Coercing people who have no symptoms of COVID-19 and have not been in contact with anyone who has – that is, the overwhelming majority of Australians – to undergo testing for SARS-CoV-2 is bad public policy and should be halted immediately.



