27 June 2022
In Part 1 of this series, I summarised the four major ways in which COVID-19 injections have interfered with the complex interactions between SARS-CoV-2 and the human immune system, then zoomed in on the first problem: the narrow and short-lived immune response that they generate.
In this post, I’m going to dig into the second major problem:
Problem #2. COVID-19 injections cause people to become susceptible to repeated reinfection with SARS-CoV-2
As was amply demonstrated by the tweets that I closed Part 1 with, repeated bouts of infection are now being normalised among those who have bought the mainstream COVID narrative. But what do the hard data say?
It’s been clear from the early days of the manufactured COVID crisis that those who contracted SARS-CoV-2 infection developed robust, broad and long-lasting immunity that provided near-complete protection against subsequent symptomatic infection (or reinfection). Dr Paul Alexander maintains a regularly-updated list of studies demonstrating the protective power of natural immunity here; as of the date of writing this article there were 153 such studies.
But, we are told by the injection pushers, “hybrid” immunity – receiving a COVID injection either before or after contracting SARS-CoV-2 infection – is even better than natural immunity! Better at preventing reinfection! Better at keeping people out of hospital! Better at saving lives! Better at making obscene profits for Big Pharma! Oh, wait, that last one just slipped out. Forget about that, and focus on all the hospital beds freed up and lives saved by the wonderful injections…
… except they weren’t. An analysis of data extracted from the Israeli Ministry of Health database on PCR-detected SARS-CoV-2 infections (for what that’s worth) and severe COVID cases in August and September 2021 – the height of Israel’s Delta wave – provides perhaps the strongest signal yet that the public has been sold a bill of goods.
The study, published in the New England Journal of Medicine in late May, 2022, included data on over 5.7 million Israelis aged over 16 years. Israel provides universal basic health coverage to its citizens, who are mandated to join one of four official health insurance organisations. Doctors and hospitals within these organisations use the same, linked electronic medical record system, which the Israeli government made “available online for use in global research” in 2018, anticipating that the move would bring in over 600 billion shekels in revenue.
“According to Prime Minister’s Office Director General Eli Groner, ‘Every doctor in Israel will be able to see the clinical files of over 98% of the population.’ The new plan, he said, will ‘unify the system and create a voluntary data bank that will draw researchers and industry here from around the world.'”
Israelis’ medical records to be put online for research
In other words, Israel’s medical data are comprehensive, up-to-date and easily accessible to researchers – the principal reason why Pfizer selected the Israeli population to be the living laboratory for its experimental mRNA injection.
Back to the NEJM study. The researchers sorted the study population into five groups:
- Those who had tested positive to SARS-CoV-2 infection before July 1, 2021 but had not received a COVID-19 injection (the “recovered, unvaccinated cohort”).
- Those who had tested positive to SARS-CoV-2 infection before July 1, 2021 and had later received a single dose of COVID-19 injection (the “recovered, one-dose cohort”).
- Those who had received a single dose of vaccine, followed by a confirmed infection before July 1, 2021 (the “one-dose, recovered cohort”).
- Those who had not been infected before the beginning of the study and who had received the second dose of vaccine at least 7 days before the start date (the “two-dose cohort”).
- Those who had not been infected before the start of the study and who had received the third (booster) dose of COVID-19 injection at least 12 days before the start date (the “three-dose cohort”).
Each cohort was further broken down into subcohorts based on how long it had been since the last immunity-conferring event (either infection or injection), ranging from less than 2 months to more than 12 months.
For the purposes of our discussion, we can ignore the three-dose cohort because there were only two months of follow-up data available at the time the analysis was conducted.
Comparing rates of reinfection in group 1 with rates of breakthrough infection in group 4, we can see from Figure 3 below that natural immunity is vastly superior to protection against infection conferred by two doses of COVID-9 injection. People who had completed their two-dose course (remember when two shots were all you needed to be considered “fully vaccinated”?) within the previous two months were twice as likely to suffer a breakthrough infection as people who had recovered from infection between 4 and 6 months ago were likely to become reinfected.
There is essentially no difference between natural immunity and either type of hybrid immunity at the 4-6 month mark, but at 6-8 months post infection/injection, group 3 is clearly in worse shape than group 1 – that is, those who got one shot then got infected were more likely to get reinfected than either those who recovered from infection and never took an injection or those who got infected and then got a shot, suggesting that the injection interfered with their ability to develop immunity against SARS-CoV-2.
(I’ve colour coded the chart below so that it’s easier to compare the subcohorts at the relevant time intervals.)
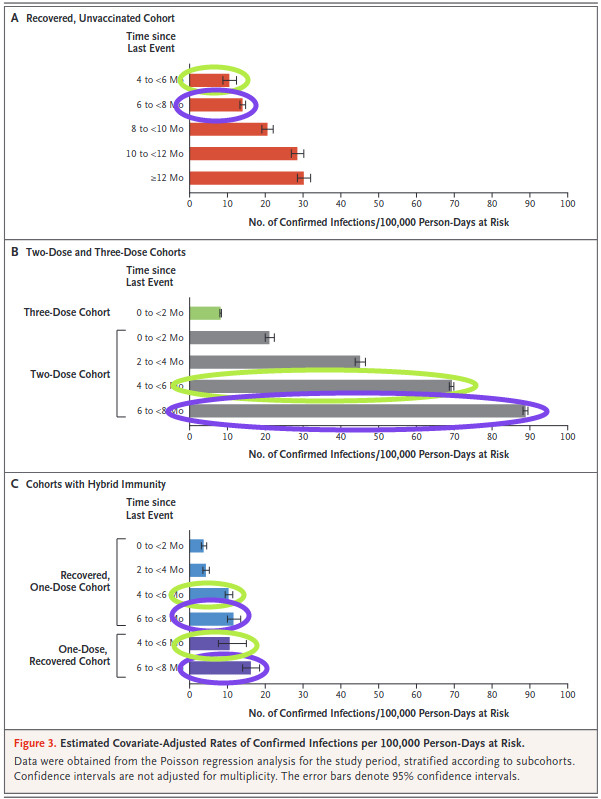
Given that infection was defined as simply a positive RT-PCR test result, with no cycle threshold defined, it’s hard to know what to make of these data. Were people who tested positive actually sick? Did they have enough virus present in their nasopharynx to infect others? We can’t tell, from this study. But since a “case” of COVID-19 has been defined throughout the entire pandemic as a positive RT-PCR test for SARS-CoV-2 (an event unprecedented in medical history), the Israeli data clearly show that COVID-19 injections are inferior to natural immunity in preventing cases.
What about clinical illness? The study used the National Institutes of Health definition of “severe COVID”: “resting respiratory rate of more than 30 breaths per minute, an oxygen saturation of less than 94% while the person was breathing ambient air, or a ratio of partial pressure of arterial oxygen to fraction of inspired oxygen of less than 300.”
Using this definition, the double-jabbed had by far the highest risk of severe disease, with little difference between the unjabbed recovered and the two hybrid immunity cohorts:
“The resulting crude rates of severe disease among persons 60 years of age or older, without consideration of the time since the last immunity-conferring event, were 0.6 per 100,000 person-days at risk in the recovered, unvaccinated cohort, 0.5 in the recovered, one-dose cohort, 0.5 in the one-dose, recovered cohort, 4.6 in the two-dose cohort, and 0.4 in the three-dose cohort.”
Protection and Waning of Natural and Hybrid Immunity to SARS-CoV-2
What about hospitalisation?
“Our data on hospitalized patients who had severe Covid-19 did not contain enough cases for a definitive analysis but did not appear to support the findings in a recent report that suggested that vaccinated persons are more protected than previously infected persons 3 to less than 6 months after an immunity-conferring event.”
Protection and Waning of Natural and Hybrid Immunity to SARS-CoV-2
So, in the middle of a supposedly deadly pandemic, not enough people ended up in hospital for the researchers to determine with any confidence which form of immunity was most protective, but they were reasonably sure it wasn’t the jab-induced kind.
And when the absurdly high risk of adverse events associated with COVID-19 injections is factored into the equation, it’s a slam dunk for natural immunity. Why would any sane person risk myocarditis, Bell’s palsy, heart attack or death for a shot that doesn’t reduce your risk of infection, severe COVID-19 or hospitalisation compared to natural immunity, and may increase all of these due to the phenomenon known as original antigenic sin (more on that later)?
The Israeli study was conducted when the Delta variant of SARS-CoV-2 was dominant. The gap between natural immunity and injection-induced immunity has widened to a chasm since Omicron became dominant, as is clearly demonstrated in the following between-country comparison.
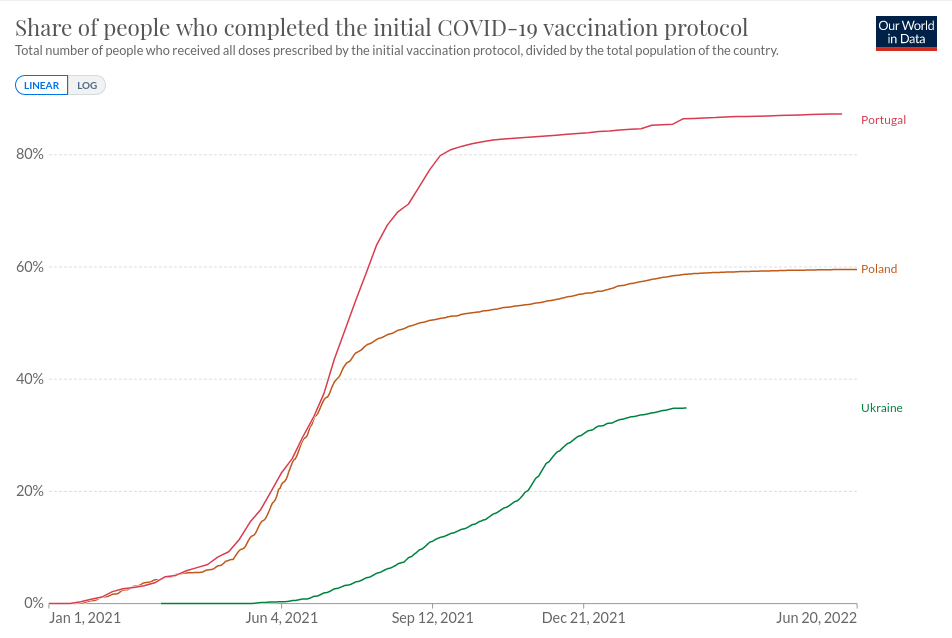
To demonstrate, let’s compare three European countries: Ukraine, its neighbour Poland, and Portugal. While Portugal is renowned as the country in which there is “no one left to vaccinate“, Ukrainians are notoriously leery of vaccines in general leading to Ukraine having one of the lowest COVID-19 injection rates in Europe. Poland is in between:
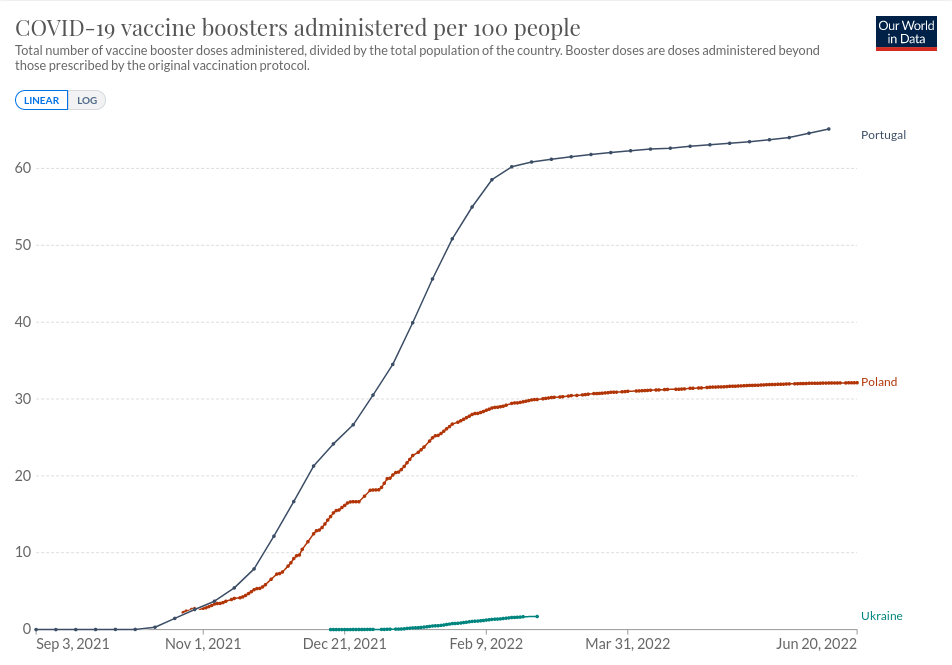
All three countries have experienced successive waves of SARS-CoV-2 infection, as each new variant exploited its evolutionary niche, but while the virus has essentially run out of susceptible hosts in the two least-injected countries, Portugal endured its highest case load after jabbing almost all its citizens, and has recently suffered an unseasonal summer spike despite rushing boosters into more than 60 per cent of them:
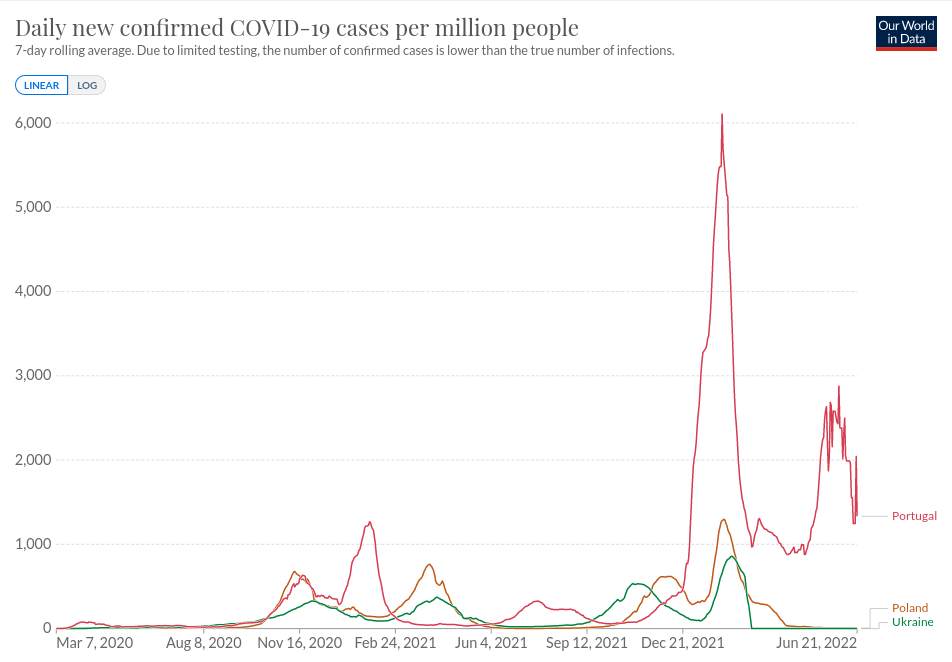
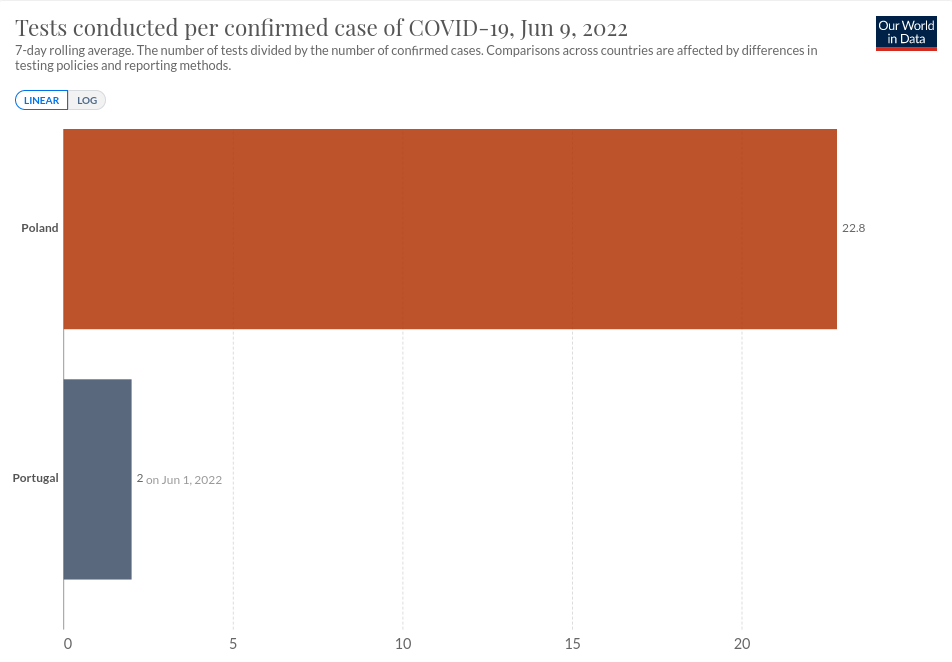
(And no, it wasn’t because Portugal was testing more aggressively, as the tests per case comparison shows:)
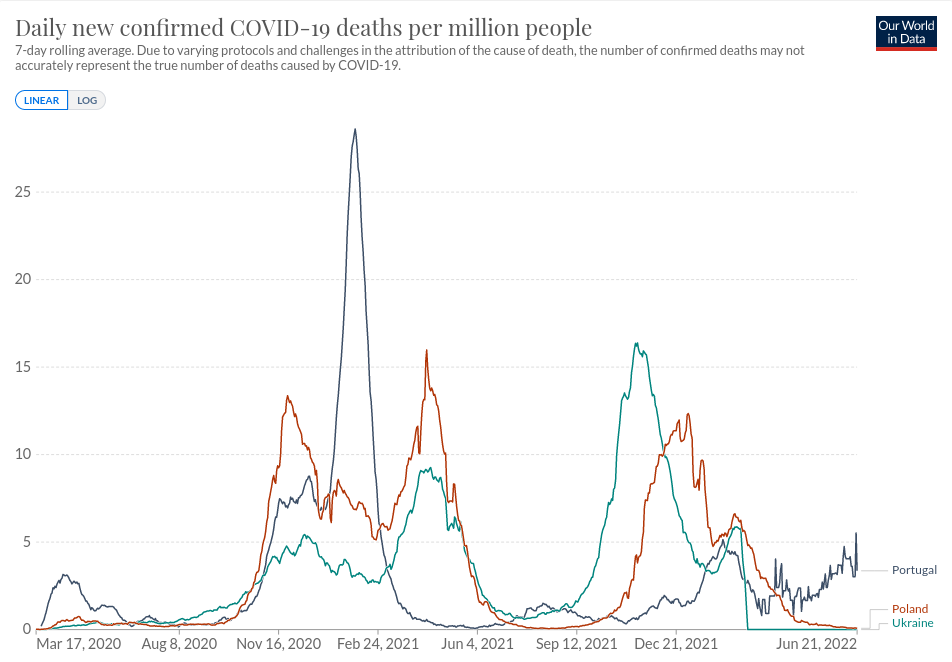
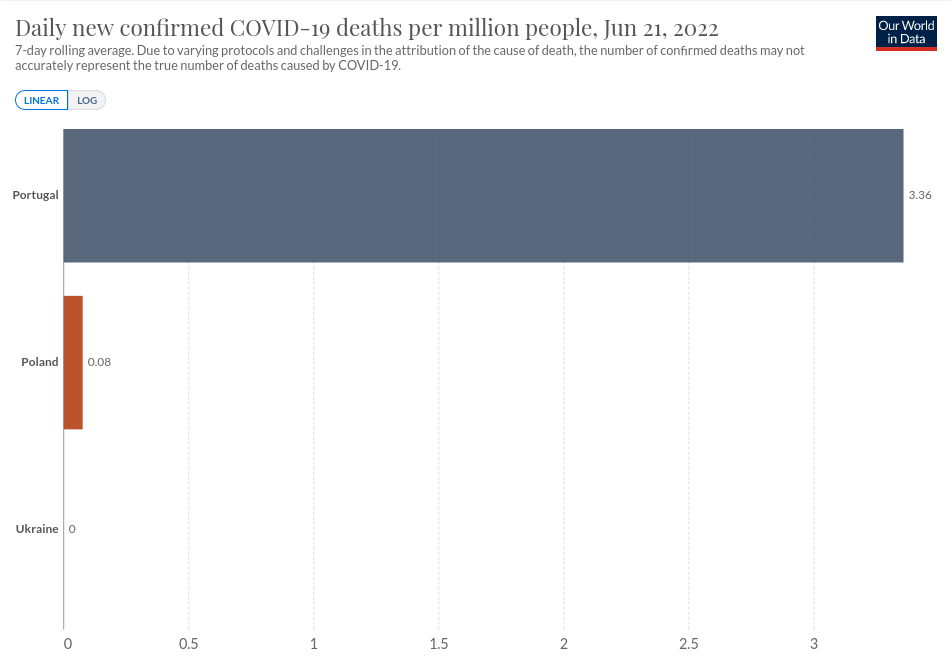
But while virtually no one is dying of COVID-19 anymore in Ukraine* or Poland, Portugal’s summer spike was accompanied by a wave of deaths which is only just beginning to subside:
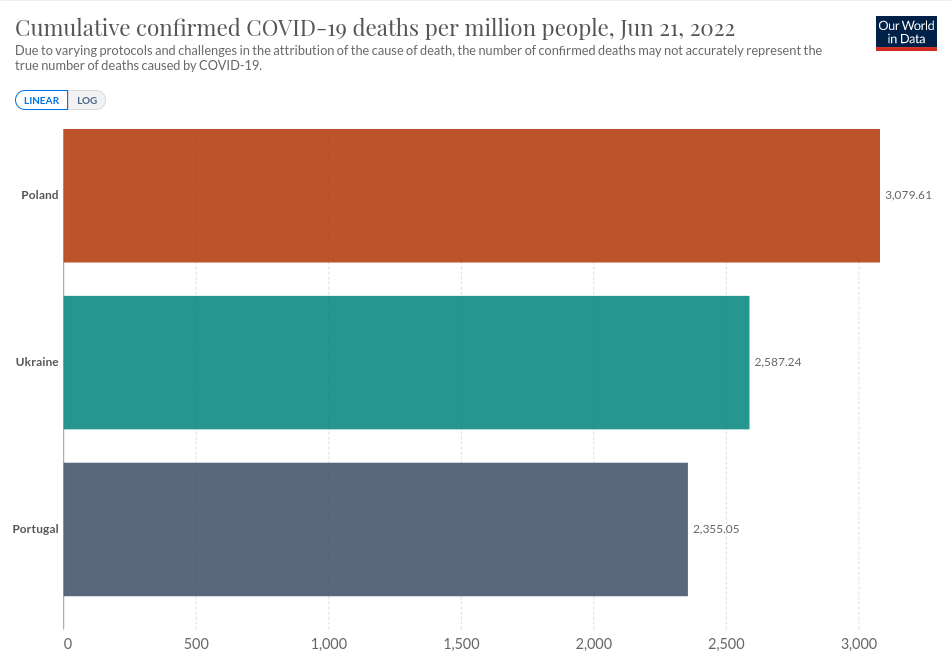
It’s not easy to eyeball the area under the curve, but when we examine confirmed COVID-19 deaths (remembering that although “deaths from” are not distinguished from “deaths with” SARS-CoV-2, no country is doing a good job of making this distinction), we see that Poland and Ukraine have cumulatively suffered more COVID-19 deaths, but Portugal is now on track to exceeding both eastern European countries:
Why are the COVID-19 injections so spectacularly failing to prevent infection and death? The most likely explanation is the phenomenon variously described as original antigenic sin, immune imprinting, antigenic imprinting and the Hoskins effect. I’ve discussed this problem in a previous article, Let’s talk about sin, baby (the original antigenic variety).
In brief, an antigen is a part of a pathogen that stimulates an immune response. As part of that response, the immune system produces both antibodies (which are like guided missiles) and activated T cells (think of these as assassins with instructions to take out only selected targets) that ‘match’ the antigen. These antibodies and T cells provide the host with immunological memory, so if the same pathogen is encountered again, it can be swiftly dispatched with highly targeted weapons.
As host and virus engage in an evolutionary arms race in which the host seeks to reduce infection whilst the virus tries to maximise it, natural mutations in the virus’ genetic code produce antigens with a slightly altered shape.
Usually, the shape change isn’t sufficiently large to evade the targeted weapons, which evolve over time to be capable of recognising many mutated versions of the virus. But in some instances, the shape alterations interfere with the ability of the guided missiles to ‘lock onto’ the antigen, leading to reduced ability of the antibody to neutralise the virus so it cannot replicate.
In the case of most viruses, the immune system adapts to the altered antigen by producing a new set of guided missiles and assassins that match it more precisely.
However, in some cases (including influenza and dengue fever), the initial exposure to an antigen – either through natural infection or vaccination – can result in the immune system becoming fixated on the form of the antigen that it initially encountered. When it ‘sees’ an altered antigen, it simply pumps out antibodies and activated T cells that match the old one. Even worse, the mismatched weapons actually inhibit the production of a new set of antibodies and T cells that would be a better fit for the new viral variant.
These antigenically fixated immune ‘weapons’ are not effective at preventing infection. In some instances they can enhance infection, causing more severe illness; this is the phenomenon of antibody-dependent enhancement which dogged earlier attempts to develop vaccines against coronaviruses.
In other instances, the opposite phenomenon, anergy, or immune non-responsiveness, occurs, resulting in recurrent infections that take longer to clear. It’s this version of original antigenic sin that appears to be occurring in the case of COVID-19.
A study published in Science on 14 June 2022 provides the strongest possible evidence yet that COVID-19 injections are inducing original antigenic sin. The researchers investigated T and B cell immunity against the Omicron variant in triple mRNA “vaccinated” healthcare workers with different SARS-CoV-2 infection histories.
It’s a lengthy and complex article, but I’ll cut to the chase: healthcare workers who had been triple jabbed produced fewer antibodies capable of neutralising the Omicron variant. Instead, their neutralising antibodies were fixated on previous versions of the virus. And those who were infected during the Omicron wave developed T cells that were active against previous variants, but not Omicron. With their immune systems unable to learn how to fight off Omicron, they are liable to becoming infected over and over again:
“Importantly, while B1.1.529 (Omicron) infection in triple-vaccinated previously uninfected individuals could indeed boost antibody, T cell and MBC [memory B cell] responses against other VOC [variants of concern], responses to itself were reduced. This relatively poor immunogenicity against itself may help to explain why frequent B.1.1.529 (Omicron) reinfections with short time intervals between infections are proving a novel feature in this wave.”
Immune boosting by B.1.1.529 (Omicron) depends on previous SARS-CoV-2 exposure
Unfortunately, jabbing these individuals with an Omicron-specific “vaccine” won’t help because it can’t overcome the immune imprinting:
“[Our finding] also concurs with observations that mRNA vaccination carrying the B.1.1.529 (Omicron) spike sequence (Omicron third-dose after ancestral sequence prime/boosting) offers no protective advantage.”
Immune boosting by B.1.1.529 (Omicron) depends on previous SARS-CoV-2 exposure
Further evidence for the induction of immune nonresponsiveness by COVID-19 injections is provided by the total failure of Paxlovid in “vaccinated” individuals, as Igor Chudov has pointed out:
“The problem is not with Paxlovid, it is the same medication as given to the unvaccinated. The problem is with the immune systems of the vaccinated. The vaccinated cannot clear Covid, while replication is temporarily paused by Paxlovid. The unvaccinated can. Why?
It is a question that I would like to explore, as it may be key to multiple reinfections of the vaccinated, as well as to “less severe disease” that the vaccinated are having, while simultaneously having higher viral loads.
Both phenomena are explained by lack of immune reaction to Sars-Cov-2 from deprogrammed immune systems that were unset and imprinted by several mRNA spike protein transfections.
Part of “severe disease” comes from cytokine storms, caused by an overreaction of immune systems. Well, if immune systems are deprogrammed, they will not overreact — not even react properly — and will not clear the virus either. They will not prevent reinfections, as well.”
We exposed Paxlovid as Snake Oil. We Won
Summing up
We now have ecological (population-level) evidence that countries with the highest rates of COVID-19 injection have higher rates of infection and death from the currently-dominant Omicron variant of SARS-CoV-2, which is the mildest strain so far. We also have high-quality retrospective cohort study evidence that getting infected with SARS-CoV-2 after receiving a COVID-19 injection is associated with a higher risk of reinfection than acquiring natural immunity with no injection. We have detailed laboratory investigations of the immune responses of triple-jabbed healthcare workers, showing that they fail to mount an appropriate defence against the Omicron variant. And we have evidence that jabbed individuals can’t clear SARS-CoV-2 infection even with the aid of an antiviral drug that appeared to be reasonably effective in unjabbed people (if you believe the Pfizer trial data).
The evidence for the manifestation of original antigenic sin known as anergy, or immune nonresponsiveness, is solid. And while the other manifestation, antibody-dependent enhancement, has not been induced by COVID-19 injections up to this point, it is becoming increasingly apparent that it’s not required for a fatal outcome; the high viral load permitted by anergy can kill too. More on that in Part 3.
* Reporting of COVID-19 cases and deaths does appear to be continuing despite the US proxy war ravaging this unfortunate nation.



