It’s not just antibiotics that mess up the microbiome – nearly one quarter of all prescription drugs adversely affect your gut bacteria.
Updated 18 August 2025
As I discussed in The Fibre Fix: How fibre-derived compounds prevent cancer, our gut microbiota perform a vast array of beneficial functions for us, including synthesising vitamins and amino acids, producing short chain fatty acids including butyrate, detoxifying bile acids, and training our immune system to tolerate food while combating harmful bacteria.
Aside from depriving our beneficial gut bacteria of the fibre they need to fuel their metabolic activities, what’s the worst thing we can do to our vast microbial workforce? If you answered, “Take antibiotics”, you’re on the right track… but it’s not just antibiotics that wreak havoc on the gut microbiome, as we’ll soon see.
Antibiotics: dropping an atomic bomb on the gut microbiome
It’s old news that antibiotics have a devastating effect on the gut microbiome. A single seven-day course of broad spectrum antibiotics such as amoxicillin, azithromycin and and ciprofloxacin, reduces gut microbial diversity (a crucial measure of the health of the gut ecosystem) by 25 per cent. The core microbiota declines precipitously, from an average of 29 bacterial taxa (individual types of bacteria) before a person takes antibiotics, to 12 taxa immediately after they complete the course.
In addition, there is a dramatic surge in a genus of bacteria called Bacteroides in the immediate aftermath of antibiotic use. Not only did the Bacteroides genus increase by 2.5-fold after one week on antibiotics, but two new Bacteroides species emerged in the core microbiota. The figure below shows how all antibiotic types flipped the ratio between bacteria in the Firmicutes phylum, and bacteria in the Bacteroidetes phylum (to which Bacteroides belong):
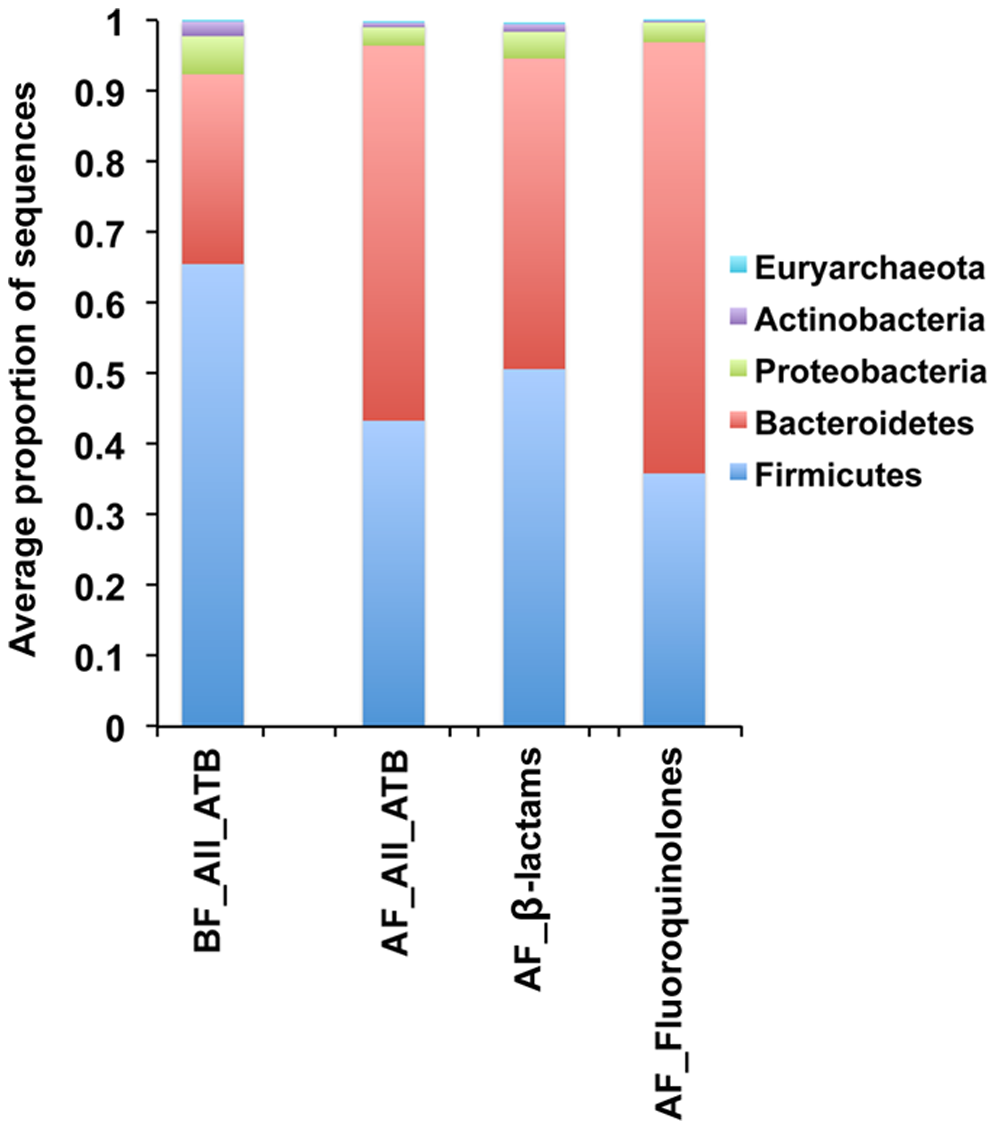
BF = Before treatment; AF = After treatment; ATB = Antibiotics. For all antibiotics N = 21; for β-lactams N = 11; for fluoroquinolones N = 10. From ‘Short-Term Effect of Antibiotics on Human Gut Microbiota‘.
Bacteroides species normally coexist peacefully alongside other bacterial taxa in the human gut, carrying out a number of useful tasks. But an overgrowth of them is associated with insulin resistance, increased body fatness and inflammation. Normally, the numbers of Bacteroides in the gut microbial community are kept in check by other bacteria which compete with them for food, and which also produce substances such as butyrate, that inhibit their growth. Unfortunately, Bacteroides taxa have greater antibiotic resistance capacity than other gut bacteria:
“Indeed, Bacteroides strains are now almost completely resistant to tetracyclines and ‘regular beta lactams’ (penicillins and cephalosporins) and moderately resistant to for [sic] moxifloxacin, clindamycin, cefoxitin and amoxicillin/clavulanic acid.”
Resistance and Virulence Features of Bacteroides spp. Isolated from Abdominal Infections in Romanian Patients
When antibiotics wipe out their competitors, the high levels of antibiotic resistance and multiple antibiotic resistance mechanisms of Bacteroides species allow them to seize the day, and stage a takeover of the gut microbiota. Once dominant, they further reduce microbial diversity and push us toward an inflammatory, insulin-resistant state. And contrary to the widespread belief that antibiotics reduce the total number of bacteria within the gut, bacterial load actually doubled after β-lactams such as amoxicillin, to which Bacteroides are highly resistant.
The devastation wrought by antibiotics can persist long after the final pill is taken. For example:
- Six months after taking ciprofloxacin, an antibiotic that is considered to have relatively minor effects on the gut microbiome, certain bacterial species that were found in patients’ guts before antibiotic treatment, but disappeared after it, had still not returned.
- A study of the long-term effects of the antibiotic clindamycin found that the gut microbiota did not bounce back to its original composition even two years after a seven-day course of treatment, with a sharp decline in the diversity of the Bacteroides community, and dominance by a small number of specific clindamycin-resistant taxa.
The consequences of extinction of species of bacteria that normally inhabit the gut are simply not known, but it is well established that any reduction in microbial diversity is associated with increased inflammation, adiposity (body fatness), insulin resistance and dyslipidaemia.
The effects of antibiotic use on the gut microbiota of babies and children is even more dramatic and persistent. Microbial diversity is low at birth, gradually increasing until around three years of age, when a child’s microbiome comes to resemble that of an adult. But early-life use of antibiotics can prevent that all-important diversity from developing in the first place. Antibiotic exposure during infancy is associated with a higher risk of childhood obesity, and of type 2 diabetes in later life.
Furthermore, antibiotic treatment increases the prevalence of antibiotic resistance genes in the bacteria that inhabit our gut. For example, a drug ‘cocktail’ of clarithromycin, metronidazole, and omeprazole is commonly used to eradicate Helicobacter pylori, a bacterium associated with stomach ulcers and increased risk of stomach cancer. This drug combination was found to cause high-level clarithromycin resistance in enterococci, a common family of gut bacteria. The clarithromycin-resistant bacteria persisted for one to three years after treatment. In other words, drugs used to wipe out one species of bacteria – Helicobacter pylori – caused other species to become antibiotic resistant.
Beyond antibiotics
Unfortunately, antibiotics are very far from being the only drugs that adversely affect our gut microbiome. Researchers screened over 1000 drugs currently on the market, for their effects on 40 strains of bacteria typically found in the healthy human gut microbiota. Of the drugs that were human-targeted – that is, not intended to combat bacterial, viral, fungal or parasitic infection – a whopping 24 per cent, across all therapeutic classes, were found to inhibit the growth of at least one bacterial strain in vitro.
The worst offenders when it came to messing with the microbiome were:
- Antineoplastics (cancer chemotherapy agents), especially antimetabolites such as 5-fluorouracil (5-FU), gemcitabine and methotrexate;
- Calcium-channel blockers, used to treat high blood pressure (hypertension);
- Hormones, including estrogens; and
- Antipsychotics, which are increasingly prescribed to children and adults who do not have psychotic illness, but have not responded to typical antidepressants.
The researchers also found that non-antibiotic drugs could promote antibiotic resistance. That is, our gut bacteria could acquire antibiotic resistance when we consume non-antibiotic drugs, putting us at higher risk of antibiotic-resistant infections. Well, that’s awesome, isn’t it?
And most worryingly, while pathogenic and multi-drug-resistant bacterial species such as Bilophila wadsworthia and E. coli were the least affected by human-targeted drugs, the gut bacteria that play the largest role in promoting human health, were the worst affected by pharmaceuticals across all drug classes:
“Species responded to drugs variably with the abundant Roseburia intestinalis, Eubacterium rectale and Bacteroides vulgatus being the most sensitive, and γ-proteobacteria representatives being the most resistant (Fig. 1a). Overall, species with higher relative abundance across healthy individuals were significantly more susceptible to human-targeted drugs (Fig. 1c). This suggests that human-targeted drugs have an even larger impact to the gut microbiome with key species related to healthy status 15, such as major butyrate- (E. rectale, R. intestinalis, Coprococcus comes) and propionate-producers (B. vulgatus, Prevotella copri, Blautia obeum) 16, and enterotype drivers (P. copri) 17 taking the heavier toll.”
Extensive impact of non-antibiotic drugs on human gut bacteria
Specific drug effects on the gut microbiota
Two systematic reviews summarised what is known about the specific effects of seven very widely-prescribed classes of drugs on the gut microbiome:
- Proton pump inhibitors (PPIs) are authorised for treatment of gastroesophageal reflux disease, but in practice are prescribed for all manner of non-specific digestive upsets.
- Metformin is prescribed to lower blood glucose in type 2 diabetics, and also used to treat women with polycystic ovarian syndrome (PCOS).
- Nonsteroidal anti-inflammatory drugs (NSAIDs) are widely used for relief of inflammation and pain – everything from headache to period pain to joint sprains. In addition, many people take a low dose of the NSAID aspirin as an antiplatelet agent to reduce the risk of heart attack and thrombotic stroke.
- Opioids are used for post-operative pain, and of course are famous for their misuse for treatment of chronic pain.
- Statins are prescribed to lower serum LDL-cholesterol.
- Antidepressants are prescribed not only to people with depression, but increasingly for treatment of anxiety, chronic pain and vasomotor symptoms associated with menopause.
- Antipsychotics, as mentioned above, are widely used not only in psychoses such as schizophrenia, but as add-ons for so-called treatment-resistant depression.
Here’s what these drugs do to the gut microbiota:
- PPIs, metformin, NSAIDs, opioids and antipsychotics were all either associated with increases in numbers of Gammaproteobacteria (including Enterobacter, Escherichia, Klebsiella and Citrobacter), or Enterococcaceae. While these are all normal inhabitants of a healthy human gut microbiota, in excess they act as pathogens, and are frequently isolated from bloodstream infections in critically ill patients.
- PPI users had clear signs of dysbiosis – imbalanced gut flora – including decreased Clostridiales and increased Actinomycetales, Micrococcaceae and Streptococcaceae. This imbalance is associated with increased susceptibility to Clostridioides difficile, or C. diff, a serious and even life-threatening gastrointestinal infection. In fact, after just 4 weeks on a PPI, patients were already manifesting microbiome changes that are associated with a predisposition to C. diff infection.
- PPIs also increase the abundance of Streptococcus, which is associated with dyspepsia. In other words, the dysbiosis induced by PPIs, may cause persistence of the symptoms that PPIs are supposed to treat!
- In addition, PPI use can cause small intestinal bacterial overgrowth (SIBO), in which certain bacteria that normally inhabit the colon (large intestine) colonise the upper gut.1
- Antipsychotic treatment resulted in a decreased ratio of Bacteroidetes:Firmicutes in the gut microbiome, mirroring trends previously seen in obese patients. This class of drugs is known to increase the risk of weight gain and metabolic syndrome.
- The selective serotonin reuptake inhibitor (SSRI) antidepressant fluoxetine increases the risk of developing Clostridiodes difficile infection.
- Diabetics taking metformin had significant decreases in the number of Intestinibacter, Coprococcus comes, Clostridium bartlettii, Eubacterium siraeum and Peptostreptococcaceae, microbial species which produce butyrate. Since butyrate improves insulin sensitivity, and type 2 diabetes is directly caused by impaired insulin sensitivity, this metformin-induced decrease in butyrate-producers is deeply concerning.
- On the other hand, metformin use was associated with a significant increase in Escherichia, Shigella, Klebsiella, Citrobacter and Salmonella enterica, bacterial species that, like Bacteroides, can have adverse effects when they overgrow. Little wonder, then, that the most common adverse effects of metformin are gastrointestinal: diarrhoea, nausea, flatulence, indigestion, vomiting and abdominal discomfort.
- People taking metformin also had elevated levels of lipopolysaccharide (LPS) – also known as endotoxin – a potent pro-inflammatory substance that crosses the blood-brain barrier, causing neuroinflammation (inflammation within the brain) and depression.
- The gut microbial profile induced by metformin use is very similar to the characteristic profile seen in people with Parkinson’s disease.
- Statins increase butyrate-producing species and decrease pro-inflammatory bacterial taxa including Proteobacteria, Desulfovibrio sp. and Bilophila wadsworthia. These microbiome-sculpting activities likely contribute to the anti-inflammatory effects of statins, which may be just as, or even more important than, their cholesterol-lowering effects when it comes to protection against coronary artery disease.
- On the other hand, statins increase the abundance of Bacteroides, which is found at higher levels in the gut of people with depression. NSAIDs also cause the proliferation of Bacteroides.
And finally, the authors of one of these reviews pointed out that reduced microbiome diversity, which is the most commonly-observed effect of drugs (even non-antibiotic drugs) that impact the gut microbiota,
“has well-documented associations with inflammatory states and diseases… [including] allergy, inflammatory bowel diseases, type 1 diabetes mellitus and multiple sclerosis, as well as colorectal cancer and metabolic disorders like obesity and T2D [type 2 diabetes] mellitus which primarily affect Western countries.”
Systematic review: human gut dysbiosis induced by non-antibiotic prescription medications
Take-aways from the research on drugs and gut bugs
Despite the voluminous amount of publications on the human gut microbiome, even the top researchers in this field freely admit that our knowledge of this ‘virtual organ‘ that is so central to human health and well-being, is still in its infancy. The studies discussed above demonstrate that commonly prescribed drugs cause extensive changes to the balance of bacteria that inhabit our guts. We can make some educated guesses about the downstream effects of these changes, based on what we know about the metabolic activities of bacterial species and the products that they produce. But without a concerted and well-funded effort to study drug-microbiome interactions and their impact on human health, guesswork is all we’ll have to go on. This is deeply concerning.
To be clear, there is no doubt that some drugs can be life saving in certain circumstances. To take just one example, penicillin is estimated to have increased survival rates from injury and infectious illness by 46 per cent, between World Wars I and II. But all too often, drugs are prescribed when they are poorly indicated, or not indicated at all, and patients are given little to no information about possible adverse effects. And even in the unlikely event that the doctor tries to give informed consent, by explaining the risks and benefits of treatment, it’s not possible to inform the patient about the implications of the drug’s effects on the microbiome, when those effects haven’t even been studied yet.
The default position should be that in non-life-threatening situations, diet and lifestyle modification is the first line of treatment. Just about every malady suffered by human beings responds well to a healthy fibre-rich diet, regular exercise, adequate rest and sleep, sensible sun exposure, nourishing social connections and a sense of purpose in life… and it’s no coincidence that your gut microbiome will thrive in these conditions too.
Concerned about the effects of drugs you are taking, or have taken, on your gut microbiome? Apply for a Roadmap to Optimal Health Consultation today to learn more, and discuss your treatment options.
- See my article The purple pill that kills for the low-down on PPIs, which are currently massively overprescribed. ↩︎



