3 June 2023
Last week’s post, New study finds all forms of hormonal contraception raise breast cancer risk, highlighted the general principle that meddling with complex systems – including women’s reproductive biology, and the sociocultural practices that have formed around its unique characteristics – will inevitably lead to negative consequences. These unforeseen side effects extended far beyond health issues (like the increased risk of breast cancer) into every aspect of human life.
The introduction of hormone replacement therapy (HRT) for the treatment of menopause-related symptoms didn’t have the profound cultural, social, economic, political and relational impact of the Pill. Nonetheless, it too was aggressively marketed to both women and men as a tool for the control of an aspect of women’s sexual biology that was socially constructed as troublesome, and medically pathologised – namely, the physical and psychological transition from the reproductive to post-reproductive phase of life.
Advertisements for HRT from the 1950s and 1960s provide a window into a world of sexism that is jaw-droppingly blatant for today’s microaggression-obsessed feminists.
Why should a man have to put up with a woman “going through the change of life” when he can ask her doctor to “make her pleasant to live with once again” by putting her on a drug made from the urine of pregnant mares?

Husbands also shouldn’t be expected to put up with their trophy wives getting old and wrinkly:
And they sure as hell shouldn’t have to put up with grumpy wives who refuse to serve them and their dinner party guests…
Even in the dying years of the twentieth century – almost four decades after the Pill catalysed second-wave feminism – advertisements for HRT in medical publications were still shaping doctors’ perceptions of menopause as disfiguring and destabilising, and encouraging them to view themselves as the potential saviours of women’s youthful attractiveness and social utility… oh yeah, and their health and stuff like that:
Both the public and the medical profession were assured that HRT would protect women against the ravages of aging, both inside and out. And it would keep them happy, cheerful, and well-adjusted to their role in society. What a relief.
But with the publication of results from the Women’s Health Initiative hormone therapy trials, in 2002, the bloom rapidly came off the HRT rose. The arm of the trial in which women who had not undergone a hysterectomy were randomised to receive either equine (horse-derived) oestrogen plus a progestin (synthetic progesterone) was halted early, because more women in the combination HRT arm developed coronary heart disease (CHD), breast cancer, stroke and pulmonary embolism (PE). These harms were not offset by the observed benefits: fewer cases of colorectal cancer and hip fracture:
“Absolute excess risks per 10 000 person-years attributable to estrogen plus progestin were 7 more CHD events, 8 more strokes, 8 more PEs, and 8 more invasive breast cancers, while absolute risk reductions per 10 000 person-years were 6 fewer colorectal cancers and 5 fewer hip fractures. The absolute excess risk of events included in the global index was 19 per 10 000 person-years.”
Risks and Benefits of Estrogen Plus Progestin in Healthy Postmenopausal Women: Principal Results From the Women’s Health Initiative Randomized Controlled Trial
While follow-up studies found that combination HRT did not decrease breast cancer mortality and that oestrogen-only HRT in hysterectomised women was associated with decreased risk of breast cancer, many women remain leery of HRT despite enthusiastic advocacy by medical organisations and some women’s health specialists (for example, Professor Susan Davis).
HRT definitively reduces the hallmark vasomotor symptoms of menopause (hot flushes, or flashes depending on which side of the pond you hail from, and night sweats). But it is also widely touted for a laundry list of other maladies that are more tenuously linked to menopause, including psychological symptoms.
For example, the Endocrine Society (which bills itself as “a global community of physicians and scientists dedicated to accelerating scientific breakthroughs and improving patient health and well being”), in its clinical practice guidelines for treatment of the symptoms of menopause, states that:
“Anxiety symptoms increase during the menopause transition and are associated with an increased likelihood of a major depressive disorder (49). ET [estrogen therapy, not extraterrestrials] may improve mild-to-moderate depressive symptoms during or shortly after the menopause transition, whereas antidepressant therapy remains appropriate treatment for major depression (50, 51).”
Treatment of Symptoms of the Menopause: An Endocrine Society Clinical Practice Guideline
Apropos of nothing at all, here are the ‘corporate liaison board members’ of the Endocrine Society:

However, a large, long-running Danish cohort study published late last year in JAMA Network Open has joined a rapidly-growing body of real-world evidence that HRT increases menopausal women’s risk of becoming depressed. And not just a little bit down in the dumps, but depressed to the point of being hospitalised.
The Danes’ highly centralised healthcare system allows them to essentially enrol their entire population into cohort studies; this is how they produced the research demonstrating a dramatic increase in the risk of being diagnosed with depression in women taking hormonal contraceptives.
This study enrolled all women in Denmark from the day they turned 45, between 1 January 1995 and 31 December 2017, excluding those who had had their ovaries removed, or been diagnosed with breast cancer or cancer in their reproductive organs before the age of 45 years. This left a total of 825 238 women, who were followed up for an average of 11 years.
The researchers identified all women who were diagnosed with depression, either as outpatients, in an emergency department, or a psychiatric ward or hospital, after entering the study. They then compared the rates of depression diagnoses in women who took no hormonal therapy, with those who had filled at least one prescription for systemic (oral or transdermal) HRT, or local (intravaginal or intrauterine) HRT.
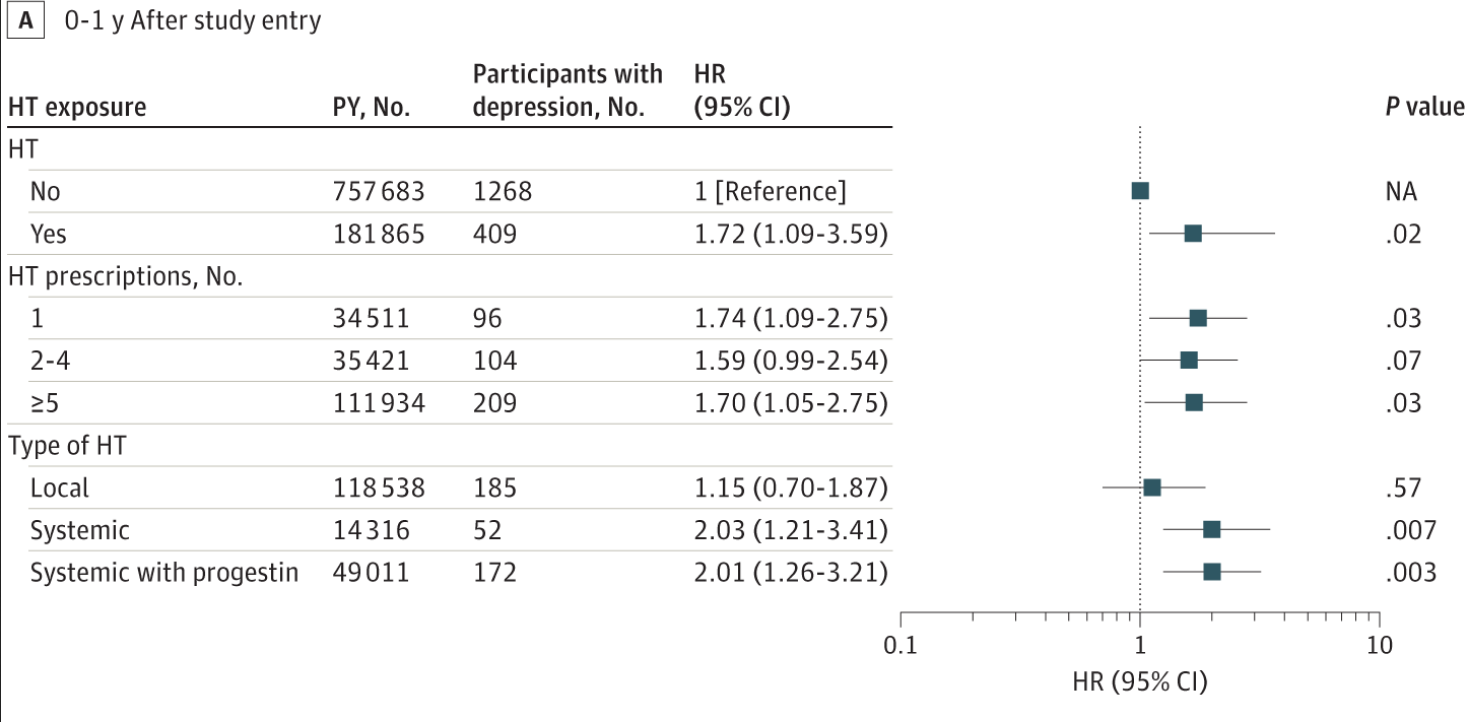
Despite being generally healthier and having substantially lower rates of prior depression (including postnatal depression) diagnoses, women who took HRT were more likely to be diagnosed with depression than those who did not, especially in the first year after commencing treatment. In fact, the risk of a new diagnosis of depression more than doubled in the first twelve months of taking an HRT pill or patch containing oestrogen alone, or oestrogen plus a progestin.
Women aged under 50 at initiation of treatment with systemic HRT had a particularly elevated risk of becoming depressed:
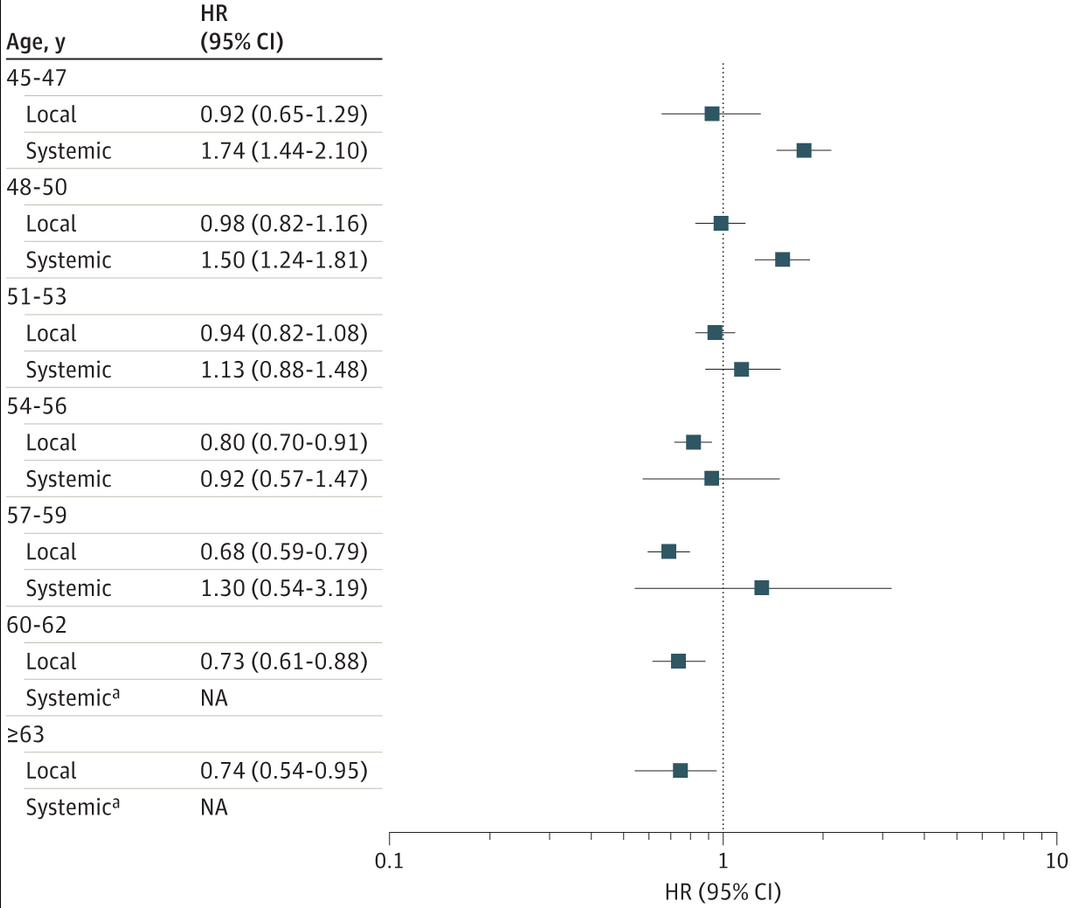
Local HRT, on the other hand, was not only not associated with depression risk in women younger than 54 years; it was associated with a lower risk of depression for those aged 54 or older. (I often recommend local oestrogen products, such as oestriol creams, for women who are experiencing vaginal dryness. This condition leads to painful sex, distressing urinary symptoms, and vaginal itching, burning and even bleeding, all of which can bring down the mood of even the most cheerful women.)
Comparing their findings to other research on the relationship between depression and menopausal hormone therapy, the authors noted a study on female US military veterans which found a 40 per cent increase in suicide attempts, and an almost two-and-a-half-fold increase in death by suicide, in women taking HRT. Studies of Finnish and Canadian peri- and postmenopausal women have also found higher rates of depression in women using hormone therapy.
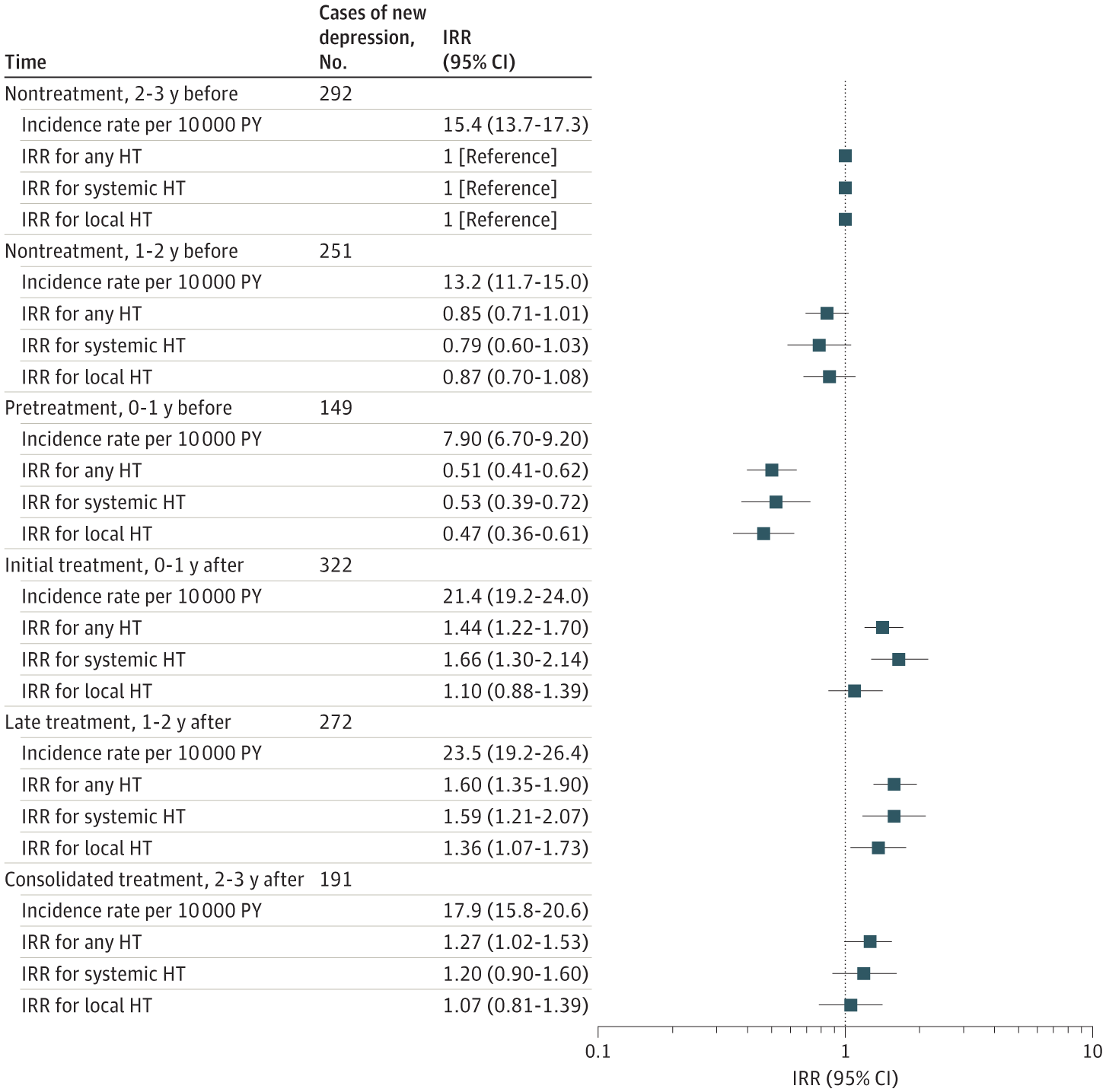
Because menopause in itself is associated with an increased risk of depression, the Danish researchers used several approaches to address potential confounding, including comparing rates of depression before and after initiation of hormone therapy. They found that the incidence rate of depression was significantly lower in the year just before women commenced hormone therapy than in the prior 2-3 years, suggesting that it was the hormone therapy, rather than menopause itself, that brought on depression:
Just as the oral contraceptive pill failed to deliver on the promise that by liberating women from the tyranny of their own fertility, it would usher them into a world of boundless opportunities for personal fulfilment (it turns out that meaningless sex with a procession of strangers, and bullshit jobs, aren’t the path to nirvana – who woulda thunk it?), the reality of HRT has not lived up to the marketing hype.
A cynic might even argue that prescribing HRT to a woman maximises her value to the pharmaceutical industry – you know, companies like the ‘corporate liaison board members’ of the Endocrine Society – by increasing the likelihood of her being diagnosed with other druggable conditions, such as depression. But we’re not cynics, are we?
So what’s a hot-and-bothered menopausal woman to do if she’s desperate for relief from unrelenting hot flushes and night sweats, but not keen on getting breast cancer or becoming depressed?
She could do a lot worse than trying out the simple intervention trialled in the Women’s Study for the Alleviation of Vasomotor Symptoms (WAVS). Just 12 weeks on a low-fat, plant-based diet which included ½ cup (86 g) of cooked soybeans daily, reduced total hot flushes by 79 per cent, and moderate-to-severe hot flushes by 84 per cent. Participants also lost an average of 3.5 kg, and reported improvements in psychosocial, physical and sexual functioning. And not one of them ended up in a psychiatric ward, or killing themselves. Well, that’s a nice bonus, isn’t it?




{kind=link}