In Part 3 of The DMSO Files, I discussed the low quality of evidence supporting the use of DMSO for both acute and chronic pain conditions, and concerns that it may interfere with tissue healing by suppressing neutrophil activity and inhibiting collagen synthesis. There is one category of chronic pain, however, for which DMSO is worth considering:
Cancer pain
Both cancer itself, and the chemotherapy, radiation, and surgery used to treat it, can cause significant pain that is not adequately relieved by any conventional pain medications – even opioids. Unsurprisingly, cancer patients with intractable pain have a significantly lower quality of life than those with no pain, or pain that can be controlled by analgaesics. Moreover, worse cancer pain is associated with shorter survival times, although it’s not clear whether this association is due to the pain itself causing cancer patients to die earlier, or whether more aggressive tumours cause higher pain levels, or whether the use of opioids to manage severe pain hastens death. Patients with terminal cancer (that is, cancer that has not responded to treatment and is expected to cause death) are more likely to have intractable pain.
And even when they’re effective, pain medications have adverse effects, which may become so intolerable that cancer patients are faced with a terrible dilemma: put up with the pain, or suffer the side effects of analgaesics, which often require the use of even more drugs. Is there a better way to manage cancer pain?
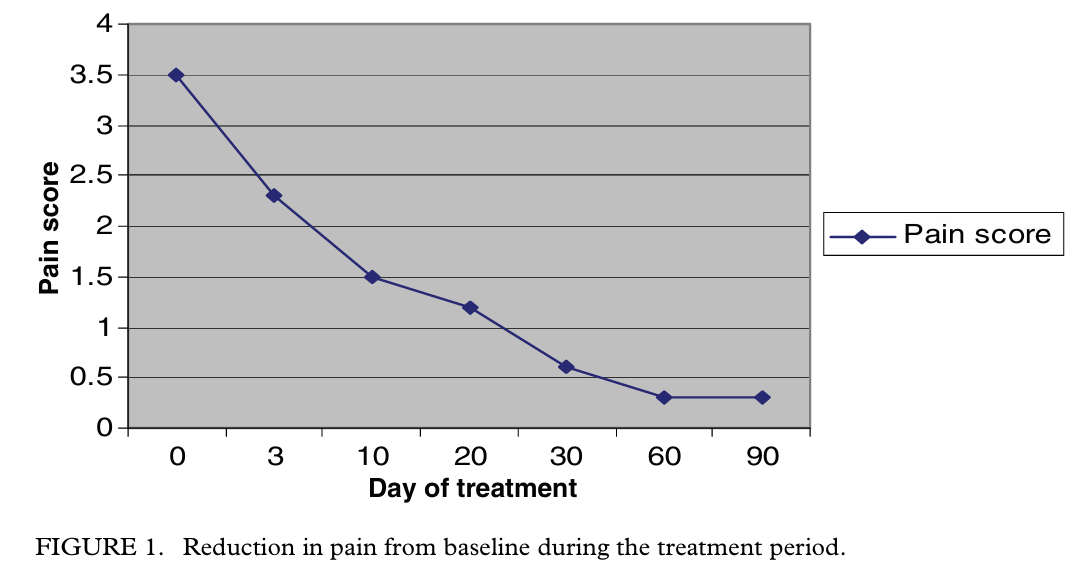
An open-label clinical study was published in 2011, of 26 cancer patients with a terminal prognosis who were ineligible for any conventional cancer treatment and who suffered from high levels of pain that was poorly managed by all guideline-approved pain medications. Intravenous infusion of DMSO and sodium bicarbonate solution led to significant reductions in pain and in use of pain medications.
The protocol comprised eight cycles of treatment, involving infusion of 20 to 60 mL of ≥99.9 per cent pure DMSO mixed with 500 mL of 1.4 per cent sodium bicarbonate, once daily for ten days with two days break between cycles (96 days of treatment in all). Dosage of DMSO was calibrated according to pain ratings, that is, patients with lower pain ratings received 20 ml of DMSO, patients with higher pain ratings received 40 ml, and patients whose pain score did not decrease after three days of treatment with 40 ml of DMSO, received 60 ml in subsequent infusions. Patients whose pain was completely controlled, were tapered down to a lower dose of DMSO in subsequent infusions.
All patients completed the treatment protocol, and by the end of the 96 days, 24 of the 26 patients had reduced their pain score by 20 per cent or more, and 25 had reduced their use of pain medications by 20 per cent or more; in fact, pain medication use dropped by an astonishing 83 per cent. Twelve patients needed morphine for pain control at the beginning of the study but by the end, no patients were using morphine.
Patients also reported fewer complaints other than cancer pain, including fatigue, headache, confusion, depression, constipation, nausea, vomiting and pruritus (chronic itch). This overall reduction in symptom burden may be explained by reduced use of pain medications that cause these symptoms, as well as by amelioration of the pain itself. No abnormalities were detected in blood chemistry, or in liver, kidney, cardiovascular or bone marrow function and in fact, these biomarkers improved over the course of the study.
The same team, led by Vietnamese oncologist Ba Hoang, conducted an open-label study in 18 patients with metastatic prostate cancer, published a few months later in 2011, this time adding magnesium sulphate to the DMSO-sodium bicarbonate solution, and 1000 mg of potassium taken orally if there was no evidence of kidney failure. One of the most difficult-to-treat consequences of metastatic prostate cancer is bone pain, for which there is no satisfactory treatment option. Reduction in pain scores obtained from the DMSO-sodium bicarb-magnesium sulphate infusions was rapid and dramatic:
All 18 patients had a 30 per cent or greater reduction in pain score by the end of the study, as well as a 30 per cent or greater reduction in pain medication use, and significant improvement in functional status and quality of life. Twelve patients had urinary outflow obstruction related to their diagnosis and treatment at the beginning of the study, while only two still suffered from this major complication of prostate cancer by the end of the 90 day treatment protocol.
Three years later, in 2014, the same team published the results of a pilot open-label study of DMSO, sodium bicarbonate, potassium chloride and magnesium sulphate infusion, combined with oral supplementation of S-adenosyl-L-methionine (SAMe, also known as ademetionine), in nine patients with advanced nonresectable biliary tract carcinomas. All patients were also advised to eliminate red meats and dairy products from their diets.
These cancers of the gallbladder and bile duct are incredibly nasty customers – poorly responsive to conventional cancer treatments and highly and rapidly fatal, with life expectancy usually measured in months. All patients had declined chemotherapy and other standard cancer treatments because of their dismal efficacy rates, high toxicity and cost. Yet not only were all nine patients still alive at the end of the six-month study, but the symptoms and biomarkers of bile obstructive syndrome and liver damage were also reversed. Liver enzymes and bilirubin dropped, weight normalised and abdominal pain, jaundice and hepatomegaly all resolved.
While the results of all three studies are very impressive, their major limitation is the open label design – that is, both the patients and the clinicians who were caring for them, knew that they were receiving the experimental treatment. With no blinding and no control group, the influence of the placebo effect on patient outcomes is impossible to assess. Patients in all three studies were allowed to continue any herbal medicines and supplements that they were taking previously, and in the third study, on biliary tract carcinomas, patients were given dietary advice in addition to the DMSO-bicarb infusions and ademetionine. The authors acknowledged these limitations and called for more research, but there has been a remarkable absence of follow-up to these potentially game-changing pilot studies of the Hoang DMSO-bicarb protocol.
Could DMSO do more for cancer patients than ease their pain?
Hoang and coauthors have also published a commentary arguing for further investigation of DMSO’s potential role in the treatment of cancer itself, arguing that the solvent is a differentiation potentiator which can reverse the process of dedifferentiation by which aggressive cancer cells are born.
Healthy cells have a distinct appearance which reflects their high degree of specialisation; liver cells have vastly different tasks to perform than muscle cells or neurons. But cancer cells have a primitive appearance that reflects their loss of specialisation… and the more aggressive the cancer cell, the more primitive its form.
DMSO is actually a component of several treatments for cancer and precancerous conditions. Mekinist, a drug used to treat melanoma and glioma, contains a low dose of DMSO to increase absorption of its active ingredient, trametanib. Two topical products applied to actinic keratoses (precancerous skin lesions) use DMSO to enhance skin penetration of their active ingredients, fluorouracil and salicyclic acid. And DMSO is used to cryopreserve T cells used in chimeric antigen receptor (CAR) T cell cancer immunotherapy (although some researchers have expressed concern that it should be removed from CAR T cells used for treatment of central nervous system tumours, due to its neurotoxicity).
But these products were formulated to utilise DMSO’s solvent and cryoprotectant properties. Might DMSO also have therapeutic effects against cancer? Hoang and colleagues summarised decades of research on tumour cell lines that suggests that DMSO, alone and in combination with other agents, promotes redifferentiation of cancer cells. Other in vitro studies found that DMSO was able to kill four human leukaemic cell lines, and that it can upregulate expression of a tumour suppressor protein, leading to reduced cancer cell growth and ability to invade neighbouring cells.
In mice with experimentally-induced lymphoma, injecting DMSO into the peritoneal cavity (the area that contains the abdominal organs) caused lymphoma cell death by apoptosis or programmed cell death, often described as ‘cell suicide’ – the orderly self-destruction of a cell in a manner that does not cause harm to neighbouring cells. And in human ovarian tumours that had been surgically removed, several chemotherapy drugs were found to have higher cytotoxicity (tumour cell-killing ability) when combined with DMSO, suggesting that patients may be able to use lower doses of chemotherapy – which means fewer adverse effects – if they take their chemo drugs with DMSO.
On the other hand, an in vitro study which examined the effect of varying concentrations of DMSO found that higher doses killed MCF-7 breast cancer cells (through both apoptosis and necrosis, which is an uncontrolled form of cell death that triggers an inflammatory response), while very low dose exposure significantly increased the cancer cells’ growth rate.
And DMSO inactivates the platinum-based chemotherapy drugs, so it must not be used in combination with cisplatin, carboplatin, or oxaliplatin. (Alarmingly, many published studies on the effects of platinum drugs have utilised DMSO as a solvent, which calls their findings into question.)
Can we draw any conclusions from the in vitro and animal studies on DMSO and cancer? Well, let me reiterate a point I made in Part 3:
“Cells removed from the body and studied in culture do not behave as cells do in a living body; and effects observed in animals often don’t replicate in humans.”
That goes for tumours removed from the body too. Cancer is a whole-body disease, and agents that kill cells in an excised tumour won’t necessarily do the same to tumour cells inside a living body. If everything that killed cancer cells in petri dishes or shrank tumours transplanted into mice, actually cured cancer in human beings, the war on cancer would have been won decades ago. So…
Should cancer patients be using DMSO?
There is simply not enough evidence to support the use of DMSO as part of a cancer treatment protocol. We have no idea how to translate the concentrations of DMSO that killed cancer cells in vitro, into dosage regimes for human beings. The dosage question is even tricker to answer given the apparent biphasic effect of DMSO, whereby high doses kill cancer cells but low doses may make them grow (at least with some tumour cell lines).
On the other hand, even absent further research, I would have little hesitation in encouraging cancer patients with intractable pain to consider DMSO-bicarbonate infusions. After all, what do they have to lose? I cannot for the life of me understand why oncologists try to dissuade patients who have a poor prognosis, little to no chance of benefiting from conventional therapies (and certainly, no hope of cure), and constant pain, from trying unconventional therapies. What’s the worst thing that could happen to terminal cancer patients, if they try a non-standard treatment – that they might die? Oh wait, terminal means the doctor believes they’re going to die anyway.1
Over my years in practice, I’ve seen multiple clients with prostate cancer that had metastasised to their bones, and the level of pain endured by these poor gents was heartbreaking. I’ve also had one client with a rapidly-progressing biliary tract carcinoma; I would not wish the end that this woman suffered, on any human being.2 If I had known about Hoang’s bicarb-DMSO treatment at the time she sought my help, I would have urged her to give it a shot. Considerations of potential longer-term harm from an experimental treatment don’t really come into play, with a person who has only months to live.
However, those potential harms do matter to people who have many years of life expectancy. I’ll be turning to the known and suspected harms of DMSO in the next instalment in this series.
Are you confused by the scientific claims and counter-claims that you encounter through popular and social media? Would you like to learn how to read scientific research, assess its biases, and understand how it fits within the body of scientific literature? My EmpowerEd membership program is custom-made for you. Activate your free 1-month trial today!
- It’s oddly reminiscent of those tragic victims of the convid scam, who confidently asserted that their dead loved ones would have been even worse off had they not taken their experimental mRNA shots. ↩︎
- Maybe Jeffrey Epstein and his merry band of child rapists deserve such an end, but I’m not convinced they’re fully human. I mean, if you put on the sunglasses from They Live and discovered that these people are actually cadaverous space aliens, would you be shocked? ↩︎



