Iron supplements: The solution to iron deficiency, or part of the problem?
In Part 1 of this miniseries on iron, I made a brief reference to the paradox that iron supplementation sets in motion processes that decrease iron absorption. Hence, people who take iron supplements because they are iron deficient, can inadvertently upregulate the pathways that caused them to have low iron status in the first place. As with so many other interventions, the supposed solution can make the problem worse. To understand why, we need to examine…
The body’s response to iron supplements
There are two key responses to iron supplementation:
- Serum hepcidin levels rise within hours of taking the supplement, and remain elevated 24 hours later. As explained in Part 1, hepcidin blocks intestinal iron absorption. So when you take an iron supplement, your ability to absorb iron from either foods, or the iron supplement you take on the following day, is reduced. At doses of 60 mg and above, fractional iron absorption was decreased by 35 to 45 per cent in iron-depleted, non-anaemic young women, 24 hours after taking the iron supplement.
- Iron supplements increase the amount of free iron in the colon (that is, iron that is not bound to a storage or transport protein), since – just as with dietary iron – most of the iron contained in the supplement is not absorbed in the small intestine, and iron supplements typically contain five to ten times as much iron as even the most iron-rich foods, such as beef liver and oysters. This unabsorbed iron causes significant shifts in the composition of the gut microbiome, as discussed in Part 1. The gut microbiota of healthy people can contain low numbers of pathogenic bacteria, but these bacteria are only able to cause disease in certain circumstances. One of those circumstances is an increase in the availability of iron, which activates virulence genes in Salmonella, Shigella and pathogenic Escherichia coli. This iron-induced dysbiosis leads to inflammation which in turn leads to increased hepcidin production and hence, reduced iron absorption.
High dose iron supplements commonly cause gastrointestinal effects including gastric upset, constipation, nausea, abdominal pain, vomiting, and diarrhoea. More serious gastrointestinal effects, including gastritis and gastric lesions, have also been reported. And at doses of 25 mg or higher, iron supplements can reduce zinc absorption and lower plasma zinc concentrations.
The key take-away is that if you’re going to take an iron supplement, it should be
- A reasonably low dose (40 mg or less)
- In a highly bioavailable form, such as iron bisglycinate chelate or ferrous ascorbate
- Taken every second day, rather than every day
- Taken in the morning, when hepcidin levels are at their lowest.
Are iron supplements the only solution to iron deficency?
Surely if a person is deficient in iron, they need to take in more iron, either via food or supplements, right? Well, it’s not always quite that simple. When dealing with iron depletion, there are three questions that we need to consider:
- Is iron intake inadequate?
- Is iron absorption compromised?
- Is iron loss excessive?
Question 1 can generally be answered by logging food and beverage intake for five days, in a food tracking app such as Cronometer or MyFitnessPal. Astonishingly, despite the near-ubiquity of iron in foods of both animal and plant origin, and the body’s ability to rapidly adapt to food sources with low iron availability (discussed in Part 1), some people manage to eat a diet so inadequate that they are genuinely not consuming sufficient iron to meet their needs. ‘Picky eaters’, elderly people with low appetites, extreme dieters and people who eat mostly low-nutrient ultraprocessed foods, can fall into this trap. Improving the diet is the obvious solution to this cause of iron deficiency, although that can be easier said than done.
Question 3 is easily answered in the case of women with very heavy menstrual periods. If you’re bleeding like a stuck pig for a week or more out of every month, your body is not going to be able to adequately compensate for the lost iron by increasing absorption. Likewise, people with inflammatory bowel disease who are passing multiple bloody bowel motions per day, and people with bleeding haemorrhoids, can rapidly run down their iron stores. Overly frequent blood donation is another obvious cause of excessive iron loss. Other causes can require more detective work. Taking aspirin and other nonsteroidal anti-inflammatory drugs, peptic ulcers, diverticulitis and colorectal polyps can all cause “occult bleeding” – chronic blood loss that is not apparent to the patient, but can usually be identified via a thorough medical history, endoscopy and colonoscopy. Addressing the condition/s that are leading to blood loss is the only long-term solution to this cause of iron deficiency, as giving iron supplements to a person with ongoing bleeding, is akin to using a teacup to bail out a boat with a giant hole in the hull.
Question 2 is the most relevant of the three to people with iron deficiency who are consuming iron-rich foods and are not suffering from excessive blood loss, and yet it’s the one that’s asked the least often. Aside from advising patients to avoid drinking tea or coffee with their iron-rich foods or supplements, most doctors and dietitians don’t consider the role that compromised iron absorption may play in iron deficiency states.
And yet, as mentioned in Part 1, by design, we only absorb a small fraction of the iron we consume (typically 1-2 mg per day), and under normal circumstances, our bodies rapidly and efficiently ramp up or tamp down the percentage of non-haem iron that we absorb, depending on our current iron status. So if you’re iron deficient, your body should absorb a higher percentage of iron from your diet, until your iron stores return to normal.
But this doesn’t always happen. To understand why, you first need to know a bit more about the proteins that regulate iron within the body, particularly those involved in the storage and transport of iron. You might remember that I touched on those proteins in Part 1, in reference to the fact that iron is far too dangerous to be allowed to freely roam through the body, and hence must be tightly encased in proteins that allow the body to make use of its chemical properties without being harmed by its reactive nature.
Following are brief descriptions of the two key proteins involved in regulating iron levels, and how they behave in various states of disease and physiological change (such as pregnancy). If you’ve ever had an iron studies blood test, I recommend pulling out your test results now, and referring to them while you’re reading this post.
Transferrin
Transferrin is a protein that picks up iron absorbed from food by cells lining the duodenum, and also from macrophages that break down worn-out red blood cells. Most transferrin is synthesised in the liver, but other tissues with a high requirement for iron, including the brain, also produce it.
Transferrin binds very tightly, but reversibly, to iron, and transports it in plasma (the liquid portion of blood) either to storage sites or to tissues that need iron for their activities. Roughly 70 per cent of the iron collected by transferrin is delivered to the bone marrow, which requires a constant supply of iron in order to produce haemoglobin within red blood cells. Transferrin is also present in the gut mucosa, where it binds iron, thus preventing gut bacteria from gaining access to it – a process known as iron withholding.
Each transferrin can bind two iron atoms in their ferric form (Fe3+). Transferrin saturation and total iron binding capacity (TIBC) reflect the proportion of transferrin that is fully loaded with iron, vs that which is carrying zero or only one iron atom, due to low iron availability. Typically, only around 30 per cent of transferrin is fully saturated with iron. When there’s not enough iron for current purposes, transferrin saturation will decrease and TIBC will increase, and vice versa.
Cells express transferrin receptors on their membranes. Transferrin delivers iron to cells by binding to these receptors and releasing the iron inside the cell. When the cell’s iron stores are low, it expresses more of these transferrin receptors in order to signal its requirement for more iron.
Increased transferrin levels are seen in
- Iron deficiency states, along with decreased transferrin saturation, and increased total iron binding capacity.
- Pregnancy, along with slightly decreased transferrin saturation, and increased total iron binding capacity.
- Estrogen-treated patients.
Decreased transferrin levels (along with increased transferrin saturation and decreased total iron binding capacity) are seen in
- Iron overload states such as hereditary haemochromatosis (although the decrease in transferrin level is modest).
- Inflammation.
- Chronic liver disease, malnutrition, renal insufficiency, and protein-losing enteropathies such as Crohn’s disease and ulcerative colitis.
- Malignancy (i.e. cancer).
- Autism.
Ferritin
Ferritin is the body’s primary iron storage protein. It maintains iron in a non-toxic, water-soluble form, within the blood, enterocytes (cells lining the small intestine), liver, spleen, skeletal muscles, and bone marrow. Each ferritin molecule normally stores around 2000 iron atoms, but can contain up to 4500.
The presence of iron triggers the production of ferritin, as does anoxia (low oxygen levels), endotoxin (a component of the outer membrane of certain types of bacteria), and cancer. Hence, although ferritin level is measured in order to assess body stores of iron, it’s an inaccurate indicator of iron status in inflammatory states.
Increased ferritin levels are seen in
- Iron overload from hereditary haemochromatosis or repeated blood transfusion.
- Liver disease, kidney disease, hyperthyroidism, high alcohol consumption, and some types of cancer.
- Inflammatory conditions (both acute and chronic – including infections and obesity) and autoimmune disorders.
Decreased ferritin levels are seen in iron deficiency and iron depletion.
Confused? This handy-dandy chart lays out the complex relationships between all these iron parameters in various disease states:
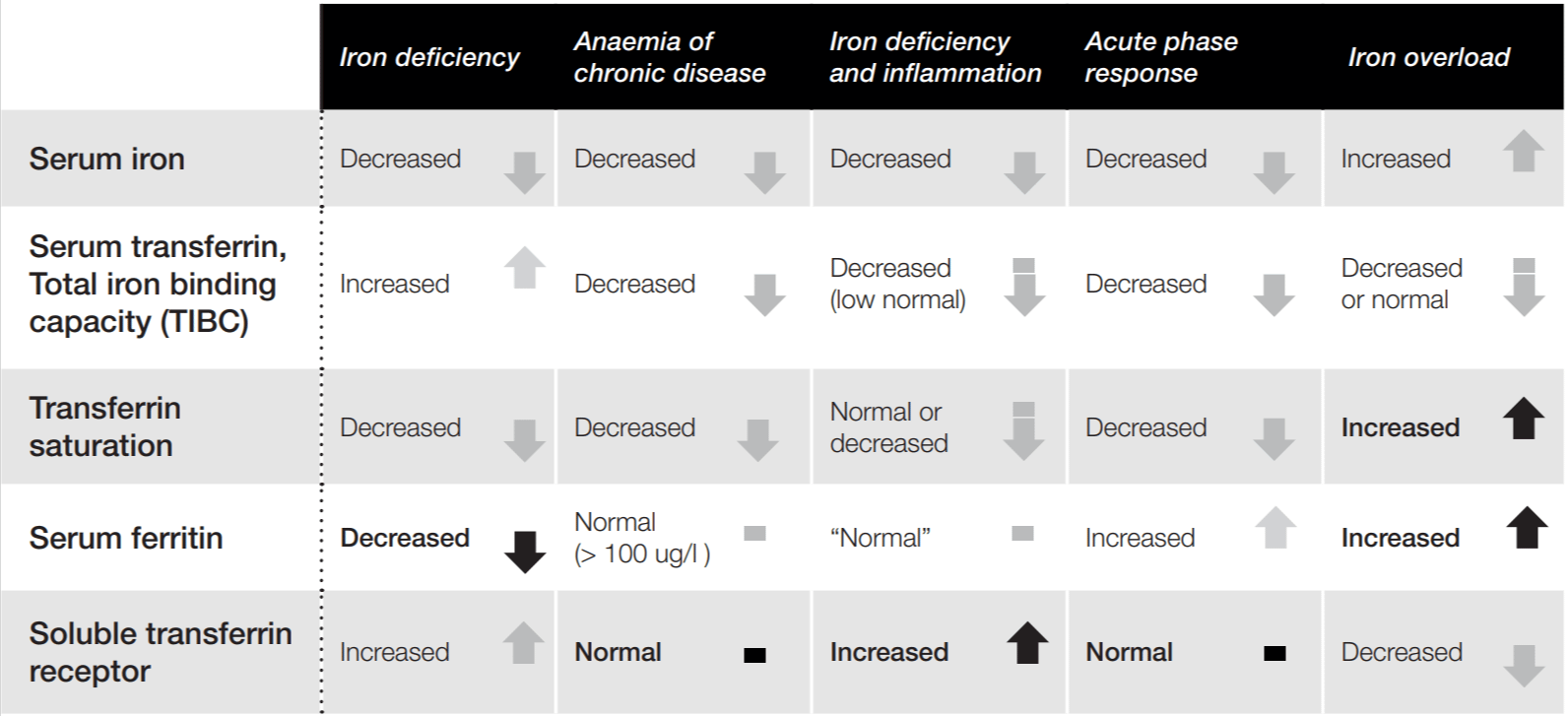
Note that the ‘acute phase response’ refers to a set of changes that occur as a result of inflammation, infection and tissue damage. And note also that in disease states characterised by inflammation, infection or tissue damage – anaemia of chronic disease1, iron deficiency coinciding with inflammation, and the acute phase response – serum transferrin and total iron binding capacity (TIBC) are both decreased. That means that the body is stifling the transport of iron to cells, even when those cells are requesting it by expressing transferrin receptors, and there’s sufficient iron stores to meet their demands.
Put this together with one of the key take-aways from Part 1 – namely, that the hormone hepcidin reduces iron absorption from the diet and prevents its release from cells that store it when the body is in an inflamed state – and a clear picture emerges: inflammation decreases iron absorption from the diet, and inhibits transportation of iron to cells, even when those cells need iron.
This might seem pretty stupid at first glance, given the centrality of iron to processes that literally keep us alive (as discussed in Part 1). But upon further reflection, this suppression of iron absorption and transport is a classic case of evolutionary mismatch – that is, a biological mechanism that increased the odds of survival in our environment of evolutionary adaptedness, but is maladaptive in the modern context.
In our hunter-gatherer forebears, the major causes of ill health were acute (i.e. of sudden and dramatic onset) and brief or self-limiting – primarily infection and injury. It makes perfect sense to curtail iron absorption and transport for a short period of time in such circumstances, in order to stifle bacterial reproduction and minimise oxidative stress-driven tissue damage. As mentioned in Part 1, most bacteria require iron for survival and reproduction, and they have some very sneaky ways to get it, including snatching transferrin in order to strip the iron from it. Ratcheting down transferrin levels, and socking iron away into storage as ferritin, as part of the acute phase response, keeps iron away from harmful bacteria, limiting their ability to cause infection.
But in the modern setting, the greatest burden of illness is from chronic conditions such as type 2 diabetes, cardiovascular disease, autoimmune conditions, endometriosis and obesity, which are characterised by low-grade, smouldering inflammation. The body’s stock-standard gambit of limiting iron availability can lead to chronically deranged iron metabolism in these conditions.
These chronic conditions are also characterised by changes in gut microbiome composition (for example, see this article on microbiome changes associated with type 2 diabetes, this one on cardiovascular disease, this one on autoimmune disease, this one on endometriosis and this one on obesity). In each case, these microbiome changes are believed to contribute to the chronic inflammation that characterises the disease condition.
And what does inflammation do to iron metabolism? Say it with me, now: inflammation reduces iron absorption and suppresses iron transport within the body. And it doesn’t have to be in-your-face inflammation; subclinical inflammation impairs iron absorption and blunts the ability of supplemental iron to reverse iron deficiency anaemia too.
The bottom line, then, is that if you have iron deficiency, with or without anaemia, or if your ferritin level (iron store) is suboptimal but not yet deficient, you should be eating a wholefood diet, rich in anti-inflammatory nutrients and phytochemicals. Non-meat-eaters need not be concerned about iron deficiency so long as they’re eating whole and minimally processed plant foods that are iron-rich, such as legumes, nuts and seeds.
You might be wondering what ‘deficient’ and ‘suboptimal’ means, in relation to iron stores. And just what is an ‘optimal’ ferritin level? We’ll cover that, in Part 3.
Are you confused by the scientific claims and counter-claims that you encounter through popular and social media? Would you like to learn how to read scientific research, assess its biases, and understand how it fits within the body of scientific literature? My EmpowerEd membership program is custom-made for you. Activate your free 1-month trial today!
- Anaemia of chronic disease occurs in certain inflammatory, infectious, and neoplastic diseases including rheumatoid arthritis, inflammatory bowel disease and blood cancers, and is the second commonest type of anaemia, after iron deficiency anaemia. ↩︎



