The copper connection
The question that drove me to start writing this miniseries on iron was, in a nutshell,
How is it possible that iron deficiency is the most common nutritional deficiency worldwide, affecting (or so we are told) 30 per cent of the global population, and well over half of premenopausal women, when iron is the fourth-most abundant element in earth’s crust and therefore ubiquitous in foods of both plant and animal origin, and the body has exquisitely finely-tuned mechanisms for increasing iron absorption from food when iron stores are low?
I mean, it doesn’t make much sense, right? And what makes even less sense is to just keep prescribing iron supplements to iron-deficient people, rather than seeking to discover, and correct, the underlying drivers of their low iron levels.
So far, I’ve discussed the roles that systemic inflammation and gut dysbiosis play in tamping down iron absorption and transportation throughout the body, and the paradoxical impact of iron supplements which also reduce the amount of iron absorbed from foods, and from subsequent iron supplements.
Now, it’s time to turn our attention to the role played by another trace metal – one which is far less abundant than iron both in the earth’s crust, and in our bodies – in the absorption and metabolism of iron. That trace metal is copper.
Copper is the 26th most abundant mineral in the earth’s crust, and the average adult human body contains just 110 milligrams – a tiny fraction of the 3-4 grams of iron that we have on board. Yet this miniscule quantity of copper plays an outsized role in regulating iron absorption and trafficking.
The role of copper-containing proteins in iron metabolism
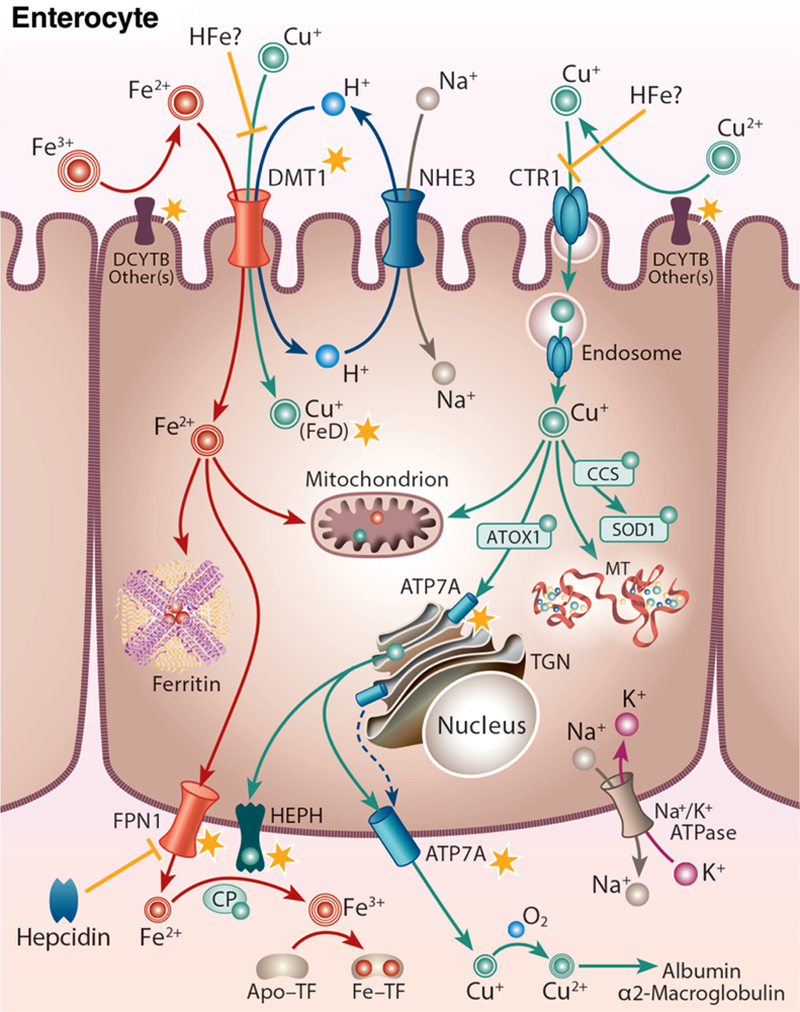
Just like iron, copper is actively absorbed (i.e. taken up by specialised receptors) by enterocytes in the upper part of the small intestine. Typically, 30-40 per cent of the copper we eat ends up being absorbed, although infants can absorb up to 84 per cent of their dietary copper intake.
Enterocytes then export iron and copper into the bloodstream so that they can be transported to cells that need them. The protein that exports iron is called hephaestin – poetically named after Hephaestus, the Greek god of metallurgy – and its activity is copper-dependent. Thus, without sufficient copper, one can become functionally iron deficient even though there is enough iron in the diet and it is being absorbed by the cells lining the small intestine.
You might remember from Part 2 that iron is transported from absorption and storage sites to tissues that need it, by a protein called transferrin. However, transferrin only binds iron in its ferric (Fe3+) form, whereas enterocytes can only take up ferrous (Fe2+) iron. The copper-containing ferroxidase (iron-oxidising enzyme) ceruloplasmin is required to convert iron into the form that can be loaded onto transferrin. Likewise, ceruloplasmin is crucial to the process of ‘recycling’ ferrous iron from worn-out red blood cells that are broken down by macrophages in the spleen and liver.
In animals experimentally deprived of dietary copper, and thus unable to produce sufficient ceruloplasmin,
“When the plasma ceruloplasmin level fell below 1% of normal, cell-to-plasma iron flow became sufficiently impaired to cause hypoferremia [low blood iron levels], even though total body iron stores were normal. When ceruloplasmin was administered to such animals, plasma iron increased immediately and continued to rise at a rate proportional to the logarithm of the ceruloplasmin dose. The administration of inorganic copper induced increases in plasma iron only after ceruloplasmin appeared in the circulation. Thus, ceruloplasmin appeared to be essential to the normal movement of iron from cells to plasma.” [emphasis mine]
The role of ceruloplasmin in iron metabolism
When there is insufficient dietary iron to meet current needs, production of ceruloplasmin normally goes up, which has the effect of mobilising iron from storage depots in order to meet the biological requirement of various tissues for iron – in particular, the bone marrow’s need for a constant supply, in order to build new red blood cells. Ceruloplasmin may also enhance iron absorption from the diet when body iron stores are depleted.
But when copper intake is insufficient, iron accumulates in small intestinal cells and iron levels in the liver become elevated. Yet serum iron and haemoglobin levels fall (i.e. anaemia develops), due to diminished ceruloplasmin activity. Brain iron concentration is also decreased by dietary copper deficiency. That is, copper deficiency induces cellular iron deficiency, even when adequate iron is present in the body. And, when copper-induced iron deficiency anaemia is ‘treated’ with iron supplements, the anaemia fails to resolve. Does this help to explain why so many individuals (especially menstruating girls and women) are chronically ‘iron-deficient’ in spite of repeated iron infusions and injections?
Quite aside from the decreased iron bioavailability induced by copper deficiency, some of the symptoms commonly ascribed to iron deficiency – especially impaired memory and concentration, and diminished immune response – may also be caused by the impact of copper deficiency on production of the thirty-plus copper-dependent proteins in our bodies… including enzymes that are required to produce haemoglobin and the red blood cells that carry it.
Speaking of symptoms induced by copper deficiency, let’s list them:
Signs and symptoms of copper deficiency
The best-known sign of copper deficiency is persistent microcytic and hypochromic anaemia – that is, red blood cells that are small and pale due to insufficient haemoglobin content, accompanied by low serum iron and low transferrin saturation – that fails to respond to iron supplementation. The accompanying symptoms include fatigue, weakness, and pallor (pale skin), which are often assumed to be due to iron deficiency.
Due to the vital roles played by copper in formation of myelin (the fatty sheath that insulates nerves) and in neurotransmitter metabolism, copper deficiency also causes neurological symptoms including:
- Peripheral neuropathy: damage to the nerves supplying the limbs, hands and feet, causing numbness, tingling, or weakness.
- Ataxia: loss of muscle control and coordination, which can impact movement, speech and swallowing.
- Myelopathy: disorder of the spinal cord, which can cause muscle weakness and gait abnormality.
- Cognitive impairment: memory problems, impaired concentration, and general cognitive decline.
- Optic neuropathy: vision loss due to damage to the optic nerve.
Other signs and symptoms include:
- Reduced bone density (osteopenia and osteoporosis)
- Neutropenia – low count of a type of white blood cell involved in fighting infection, leading to impaired immune function
- Diarrhoea
- Cardiac hypertrophy (abnormal thickening of the heart muscle)
- Weak connective tissue
- Depigmentation of hair.
It has also been suggested that low copper status may be linked to Alzheimer’s disease, ischaemic heart disease and myelodysplastic syndrome (a type of blood cancer), although confirmatory evidence is needed to firmly establish the link.
What causes copper deficiency?
Overt copper deficiency is considered to be rare in healthy individuals. Risk factors include:
- Malabsorption syndromes, such as coeliac disease, Crohn’s disease and bariatric surgery-induced malabsorption
- Long-term total parenteral nutrition (intravenous feeding)
- Prolonged diarrhoea
- High dose zinc supplementation (as excessive zinc intake causes reduced copper absorption)
- … and, finally and somewhat ironically, excessive dietary iron intake from food and supplements.
However, suboptimal intake of copper is more common than is generally acknowledged, with half of the adult population consuming less than the amount recommended by the European and United Kingdom nutrition advisory bodies. Analyses of the nutritional content of various crops across time reveals that copper levels in fruits, vegetables, high-yielding wheat cultivars and meat declined over the course of the twentieth century. In fact, copper deficiency is the leading nutritional deficiency in farmed animals worldwide.
Glyphosate, the widely-used herbicide, may be one of the culprits causing declining levels of copper (and other elements including iron, manganese, zinc, and nickel) in our food, as it is a chelating agent which binds to minerals, inhibiting their uptake by plants.
The fortification with iron of many refined grain products – including many breakfast cereals and some white breads – creates a double-whammy with the declining copper content in our food. Without sufficient copper, our ability to absorb and utilise iron, whether it’s naturally-occurring or from fortification, is impaired. And shovelling in more iron via food fortification or supplements only exacerbates the copper deficiency, which in turn worsens the functional iron deficiency, in an endlessly spiralling doom loop.
So how can we tell if we’re copper-deficient?
The body maintains tight homeostatic control over copper levels in the bloodstream, so it’s a challenging nutrient to assess for either deficiency or overload states. Animal experiments have established that the most accurate way of assessing copper status is to measure liver copper, but since this is done post mortem, it’s not exactly practical.
Serum copper is the best available marker of copper status currently known, but it’s not sensitive enough to detect copper inadequacy as opposed to frank deficiency or overload states. Ceruloplasmin concentrations are reduced in severe copper deficiency, but again, not in mild copper undernutrition.
Furthermore, both serum copper and ceruloplasmin are acute phase reactants, meaning that they rise in response to infection and inflammation, limiting their usefulness for assessing copper status in people already in ill health.
The bottom line is that it’s actually pretty difficult to determine whether copper insufficiency is contributing to low iron status (or to any other health problems) in all but the more severe cases. But if you suspect that low copper might be an issue for you, here’s what you can do to test the hypothesis:
- Stop taking iron supplements, at least temporarily. Check any multivitamins or combination nutritional supplements to make sure they don’t contain iron.
- Avoid iron-fortified foods. You’ll need to read the ingredients list; if iron is added to the product, it will be clearly indicated.
- Stop taking zinc supplements.
- Buy organically-grown foods whenever possible – especially in the case of crops that, when grown conventionally, are routinely sprayed with glyphosate, and the animals that are fed these crops. In Australia, glyphosate is registered for late-crop use (i.e. five to seven days before harvest) on wheat, canola, and legumes including adzuki beans, chickpeas, cowpeas, faba beans, field peas, lentils, lupins and mungbeans. Much of these crops ends up as stockfeed, which no doubt helps to explain widespread copper deficiencies in farmed animals.
- Include copper-rich foods in your diet every day. Oysters, crab meat and liver are the richest sources, but are also heavily contaminated with persistent organic pollutants – even organically-reared beef, chicken and lamb. Organically-grown seeds (especially sunflower seeds), nuts, legumes, mushrooms (especially shiitake) and cocoa are particularly rich sources.
Of course, people with Wilson’s disease or any other copper overload disorder need to minimise their copper intake, and should follow the advice of their health care practitioner.
Finally, I don’t recommend taking copper supplements unless you are under the guidance of a health practitioner who is carefully monitoring your copper, zinc and iron status… and even then I would have concerns. The problem with supplements is that they aren’t packaged in the nutritional matrix of food, and therefore they don’t behave like the nutrients that we consume in food. That’s not to say that supplements are never appropriate, just that they should only be used when a clear need is established, there is strong evidence from clinical studies conducted in human beings to support their use, and the person taking them is being monitored for adverse effects.



