I’ve banged on quite a lot about informed consent on this blog (see here, here, here, here, here, here, here, here, here, here, here, and here) and for good reason: informed consent is the ethical foundation of health care. A concise definition of informed consent is as follows:
“Informed consent is a process in which a healthcare professional educates a patient about the risks, benefits, and alternatives of a given procedure or intervention.”
Informed consent
Practitioners who do not give informed consent about the risks of treatment with DMSO are, by definition, practising unethically, whether they’re recommending it to their patients or spruiking it online. In previous instalments of this series, I’ve mentioned a few of those risks in passing, including suppression of the neutrophil response, acceleration of collagen breakdown and inhibition of its production, and stimulation of the growth of certain breast cancer cells. Let’s take a deeper dive into the hazards of DMSO, from the trivial to the serious and even life-threatening.
Minor adverse events
The most common side effect of topical application of DMSO is skin irritation. Many people experience a burning, stinging or itching sensation that is generally transient (usually lasting between 1-24 hours), although early proponents of DMSO reported that some of their patients were so sensitive that they could not tolerate the skin irritation and had to discontinue treatment. Roughness, blistering and peeling of the skin occur quite commonly; other reported skin effects include flushing, rash, paraesthesia/burning sensation, thickening of the skin, increased pigmentation and bullous dermatitis.
The other most commonly-reported minor side-effect is a distinctive taste in the mouth and a breath odour, usually described as garlic-like or clam-like or oyster halitosis. The malodorous breath is due to exhalation of dimethylsulphide, a metabolite of DMSO. While merely bothersome to most, an early clinical report noted one case in which the emphysemic husband of a woman who was using DMSO topically, became short of breath just from being in the same room as her.
Systemic reactions
Headaches, dizziness, trembling, nausea, acne, generalised dermatitis and urticaria (hives), fatigue and lethargy occur more rarely, although in one early clinical report, 7 per cent of patients treated with topical DMSO for musculoskeletal disorders had to discontinue treatment due to “local dermatitis, generalized dermatitis, or extreme lethargy”.
At a relatively high dose of 1 g DMSO per kg of body weight, applied topically, over half the experimental subjects (52 per cent) experienced sedation, 42 per cent suffered headaches and 32 per cent became nauseous.
Severe allergic reactions have been reported, although rarely.
Using DMSO topically or intravenously, or taking it orally, can cause dizziness, drowsiness, nausea, vomiting, abdominal cramping, diarrhoea, constipation, decreased appetite, hypo- and hypertension (low or high blood pressure), bradycardia (abnormally slow heart rate), tachycardia (fast heart rate), ventricular extrasystoles (irregular heartbeat), chest discomfort/tightness, cough, dyspnoea (difficulty breathing), lung oedema and pelvic pain.
DMSO causes haemolysis (breakdown of red blood cells) when introduced into the blood at higher than 50 per cent concentration and hence, intravenous use may aggravate blood disorders such as haemolytic anaemia.
A systematic review of 109 studies reporting on the use of DMSO via topical, oral, intravenous and intravesical (injection into the bladder) routes of administration reported that gastrointestinal and skin reactions were the most commonly reported adverse effects, and that most adverse effects were mild and transient.
Inactivation of drugs
As discussed in Part 4, DMSO inactivates platinum-based chemotherapy drugs, so it must not be used in combination with cisplatin, carboplatin, or oxaliplatin.
It also inhibits the conversion of sulindac, a nonsteroidal anti-inflammatory drug used for osteoarthritis, rheumatoid arthritis, ankylosing spondylitis and other inflammatory conditions, to its active form, rendering it ineffective.
Enhancement of drug and chemical toxicity
DMSO’s ability to penetrate the skin and cellular membranes, and to enhance the absorption of other substances, is a double-edged sword. When used topically, orally or intravenously, it can increase the absorption and pharmacological activity of drugs, heightening the risk of toxicity. In the case of blood thinners, steroids and sedatives, the results could be serious or even fatal – especially since DMSO may already slow down blood clotting by inhibiting platelet aggregation.
By inhibiting acetylcholinesterase, an enzyme that breaks down the neurotransmitter acetylcholine, DMSO increases acetylcholine levels. Among its other roles, acetylcholine is involved in involuntary muscle movement. When used along with drugs that also upregulate acetylcholine activity, such as the Alzheimer’s drugs donepezil and galantamine, and pilocarpine and carbachol, used for glaucoma, DMSO can increase the risk of cholinergic side-effects such as bradycardia, bradypnoea (abnormally slow breathing rate), cramps, muscular weakness, paralysis, fasciculation (muscle twitching), diarrhoea, and blurry vision.
As mentioned above, DMSO interferes with the bioactivation of sulindac, but the combination of the two drugs has been reported to cause “profound mixed sensorimotor peripheral neuropathy”, meaning damage to the sensory and motor nerves, which did not fully resolve after discontinuation after treatment.
The combination of alcohol and DMSO doubles the level of psychomotor impairment and slowed nerve conduction caused by alcohol alone, so you definitely shouldn’t combine drinking, DMSO and driving!
And DMSO will also enhance absorption of anything present on the skin – such as topical medications, personal care products, cleaning chemicals or microplastics from clothing – again potentially leading to unexpected adverse effects or interactions and long-term harms. Industrial-grade DMSO can itself contain impurities that can be absorbed through the skin; it should never be used for medicinal purposes.
Epigenetic effects
As mentioned in Part 1, the first medical use for DMSO was as a cryopreservation agent for red blood cells and sperm. DMSO is so good at protecting cells from the damage caused by ice crystal formation during freezing, that it became widely used for cryopreservation of human oocytes (egg cells), sperm cells and embryos used in in vitro fertilisation (IVF).
However, more recent research has raised urgent questions about the epigenetic effects of DMSO on gametes and embryos, and how these might impact on the health of babies born through IVF and other assisted reproductive technologies.
In 2019, researchers used 3D InSightTM Human Cardiac Microtissues and Human Liver Microtissues to evaluate the biological effect of DMSO on genetic expression. These three-dimensional microtissues, derived from human-induced pluripotent stem cells, are advanced models used for studying the function of human organs and the disease processes that affect them. They provide a far more realistic representation of tissue function than traditional two-dimensional cell cultures, allowing for more accurate drug testing and disease modelling.
At a concentration of just 0.1 per cent, DMSO induced profound changes in the transcriptome (the gene readouts present in a cell), proteome (the proteins expressed by a cell) and DNA methylation profiles (gene expression and regulation patterns) of both the heart and liver microtissues, with grave implications:
“In both tissue types, transcriptome analysis detected >2000 differentially expressed genes affecting similar biological processes, thereby indicating consistent cross-organ actions of DMSO. Furthermore, microRNA analysis revealed large-scale deregulations of cardiac microRNAs and smaller, though still massive, effects in hepatic microtissues. Genome-wide methylation patterns also revealed tissue-specificity. While hepatic microtissues demonstrated non-significant changes, findings from cardiac microtissues suggested disruption of DNA methylation mechanisms leading to genome-wide changes. The extreme changes in microRNAs and alterations in the epigenetic landscape indicate that DMSO is not inert. Its use should be reconsidered, especially for cryopreservation of embryos and oocytes, since it may impact embryonic development.”
‘DMSO induces drastic changes in human cellular processes and epigenetic landscape in vitro‘
Another study examined the effect of DMSO on the transcriptome of egg cells of healthy women undergoing elective oocyte cryopreservation (egg freezing). Half of each woman’s oocytes were vitrified (rapidly frozen) using a DMSO-containing cryoprotectant, while the other half were snap frozen in phosphate buffer. 26 per cent of the 27,837 total genes identified were differentially expressed in the DMSO-treated egg cells, with significant dysregulation of genes involved in mitochondrial function, insulin signalling, sexual differentiation, and multiple pathways involved in growth and in cancer.
Babies conceived through IVF are more likely to be born premature, to suffer from birth defects, and to have low birth weight, growth and metabolic disorders, genomic imprinting diseases, psychomotor/mental developmental delays, early childhood cancer, and early-life cardiovascular and metabolic risk factors that may ultimately lead to chronic cardiometabolic disease. The usual explanations for these abnormalities are increased parental age and the processes underlying infertility itself, but these studies provide compelling evidence that DMSO may also be a contributing factor.
Toxic effects on cells
Aside from assisted reproductive technology, the other major application of cryopreservation agents is in the field of organ and cell transplantation. DMSO is used to cryopreserve stem cells and bone marrow for transplantation, and studies of toxicity associated with receiving such transplants has prompted research into the mechanisms by which DMSO damages certain cell types.
DMSO toxicity occurs in approximately one in every 70 stem cell transplant recipients, causing fatal arrhythmias (heart rhythm abnormalities), respiratory arrest with diffuse alveolar haemorrhage (bleeding in the air sacs of the lungs), seizures, leukoencephalopathy (disease affecting the white matter of the brain) and haemoglobinuria (presence of haemoglobin in the urine, indicating breakdown of either red blood cells or muscle cells).
The haemolytic effect of DMSO on red blood cells was discussed above, and can occur in vitro at concentrations as low as 0.6 per cent. Likewise, the previously-discussed effects of DMSO on cardiac microtissues may explain the heart rhythm disorders observed in DMSO toxicities.
What about the DMSO-induced neurological toxicity? In vitro studies of astrocytes – the workhorses of the central nervous system – found that a 1 per cent solution of DMSO caused mitochondrial damage, reactive oxygen species production (i.e. oxidative stress), and impaired function of the excitatory neurotransmitter glutamate (which is involved in seizures), while a 5 per cent solution caused astrocytes to ‘commit suicide’ through apoptosis. And in both in vitro and in vivo studies of developing mouse brains and neurons, very low concentrations of DMSO – in line with those experienced by children undergoing bone marrow transplantation for paediatric cancers – caused widespread neuronal death. Likewise, very low concentrations of DMSO were found to be toxic to the retinal neurons of rats, again primarily via inhibition of mitochondrial function.
Finally, it has been suggested that DMSO’s anti-inflammatory and antioxidant effects are actually attributable to its toxicity to two types of white blood cells – T cells and monocytes – that are involved in the inflammatory response to cell damage and infection.
Conclusion
Proponents of DMSO play down its potential hazards, but the researchers who have documented its toxic effects on many different cell types, are not so sanguine. As the authors of the study on rat retinal neurotoxicity stressed,
“DMSO is a universal solvent routinely used in experimental and biological disciplines, and is widely accepted to be nontoxic at concentrations 10% (v/v…). It is often used to solubilize drug molecules that are otherwise poorly soluble. Our finding that at concentrations 10% (v/v), DMSO is toxic is unexpected. These results underline safety concerns of using low concentrations of DMSO as a solvent for in vivo administration of numerous molecules, which we show not to be safe. We believe that the scientific community should question the use of DMSO in biological assays, with particular relevance to delivery to neuronal cells. Finally, due to the broad number of drugs dissolved in DMSO, we believe these results have widespread implications, not only in the eye and in neuroscience, but also throughout the whole body.”
‘Unexpected low‐dose toxicity of the universal solvent DMSO‘
Occasional topical use on small areas of the skin and for short periods of time are unlikely to be hazardous, although there’s always the risk of severe allergic reactions. But we just don’t know what long-term use of DMSO does to the human immune system, central nervous system, musculoskeletal system and cardiovascular system. What we do know, from cell culture and animal experiments, raises serious concerns; with chronic use, it is virtually inevitable that some people will reach their personal toxic threshold.
This danger is magnified by the current craze for using DMSO for every ailment known to humankind, topically, intravenously and by mouth. Geoff Pain has pointed out that adverse event reports for DMSO surged in 2025 (when online ‘health influences’ began heavily promoting it):
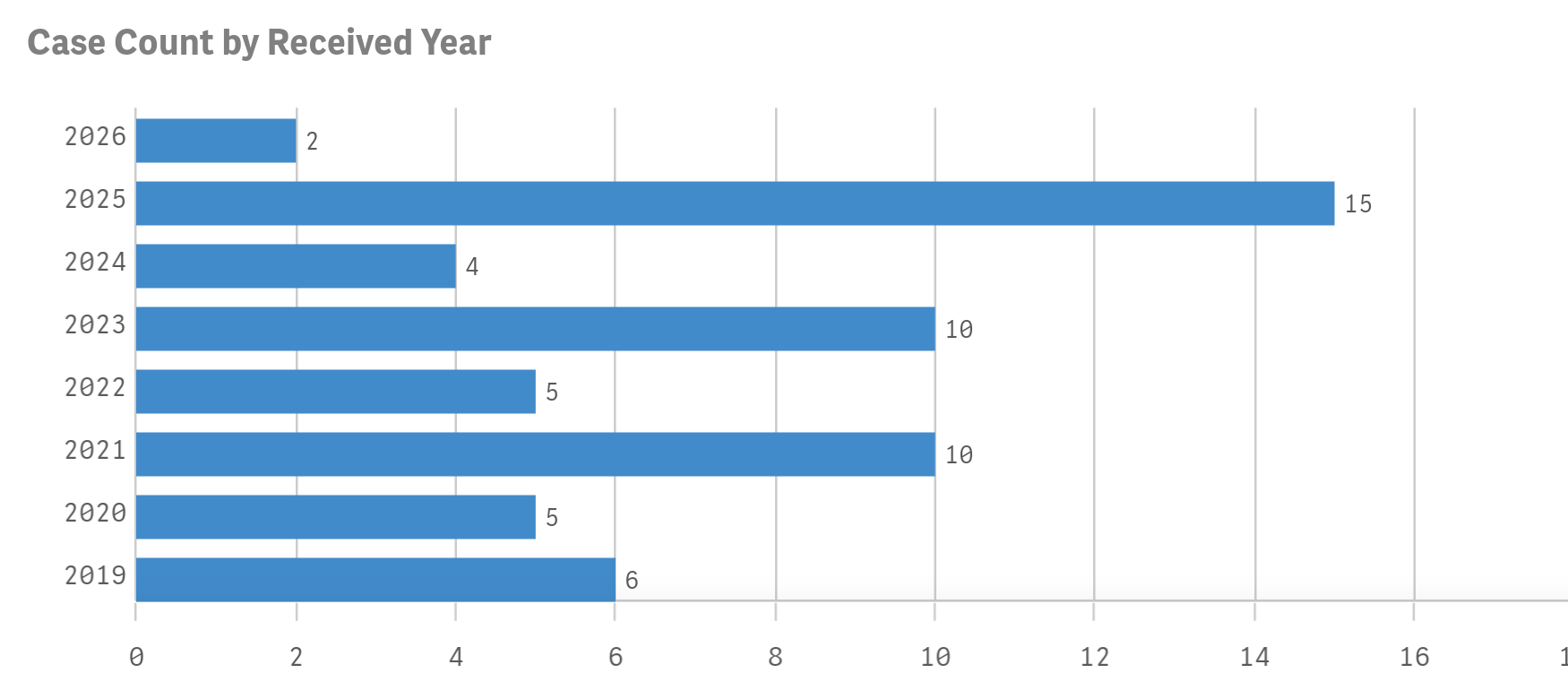
… and that the death to adverse event report ratio is high, at 9.86 per cent (as of February 2026).
Finally, pregnant and breastfeeding women should definitely not use DMSO, given the potential dangers to the foetus and infant uncovered by both IVF studies and animal experiments.
If you still want to try DMSO after learning about its risks, that’s your decision. Just make sure you’re making an informed decision, rather than an emotional one, swayed by the hyperbolic claims of DMSO promoters.



